Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 61-year-old male presented to his physician with a history of symptoms, beginning about three weeks after he returned from a trip. Symptoms included general malaise, followed by fever, chills, headaches and back pain. The man lived in southern Texas and had returned from a photographic safari to Africa, including Kenya, Tanzania, Uganda, and South Africa. He had seen a physician prior to returning to the United States and had received some antimalarial medication. He was an active wildlife photographer and was often exposed to a number of life zones and resident plants, animals, insects, etc., both at home and on trips outside of the United States.
Although both the patient and several others in the group remembered being bitten by insects, he was the only one who was symptomatic. On examination he was found to have several swollen areas, including a lymph node on his neck and a draining lesion on his upper arm.
Blood was drawn for routine hematology procedures and a specimen was also drawn to be sent to microbiology for examination as blood films stained with Giemsa stain. Based on his travel history, additional laboratory revealed a slightly elevated white blood cell count with a relative lymphocytosis. His gamma globulin level was elevated with a marked elevation of the IgM.
Please comment on the possible diagnosis related to the history of insect bites, the patient's clinical symptoms and the relative travel history. Routine examination of thin blood films revealed the following:
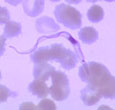
1. Thin blood film |
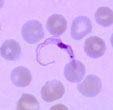
2. Thin blood film |
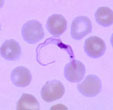
3. Thin blood film |
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #9
The images presented in Diagnostic Quiz #9 are the following:
Comment: This was a case of African trypanosomiasis, probably caused by T. b. rhodesiense (East African Trypanosomiasis) based on travel history (Kenya, Uganda), the severity of symptoms, and overall description of the case. Although the man lived in southern Texas where Trypanosoma cruzi is found (cause of Chagas' disease, American Trypanosomiasis), the African trypomastigotes and the American trypomastigotes look quite different.
Trypanosoma cruzi |
Trypanosoma b. rhodesiense |
Comments:
The African trypomastigotes (both East and West African trypomastigotes) (see right photograph above) have a very small kinetoplast (the dot at one end of the organism), while T. cruzi tends to have a very large kinetoplast that appears to go beyond the body of the organism (see left photograph above). Both organisms can actually be in a "C" shape; this configuration alone does not indicate infection with T. cruzi.
The course of infection in African trypanosomiasis occurs in three stages. Soon after inoculation of the metacyclic trypanosomes by an infected tsetse fly, an inflammatory lesion develops at the site of inoculation; this lesion is called the trypanosomal chancre. Trypomastigotes then invade the local lymphatics and later the bloodstream. After a time, the organisms invade the choroid plexus and enter the brain and cerebrospinal fluid (CSF). There is quite a bit of variation between the two diseases caused by East African and West African trypanosomiasis. In the East African disease (T. b. rhodesiense), chancres are common, the hemolymphatic stage is severe, and rapidly progresses to a fatal meningoencephalitis, often within months of infection. With the West African form of the disease (T. b. gambiense), chancres are uncommon, the hemolymphatic stage may not be seen, and meningoencephalitis progresses very slowly, often over several years, thus the "sleeping sickness" syndrome.
During the course of the infection, the number of trypomastigotes in the blood fluctuates. This relapsing parasitemia is due to the host's immune response to the parasites. Each decline in parasite number results from the antibody-mediated destruction of trypomastigotes bearing a particular variant surface glycoprotein (VSG). Each new wave of parasitemia represents the growth of a trypomastigote population expressing an antigenically different VSG. This process of ANTIGENIC VARIATION is a feature of all African trypomastigotes. Since each trypomastigote expresses only one VSG at a time and has as many as 1,000 different VSG genes, the number of different variable antigen types (VATs) that can be expressed during an infection is quite large. The continued response of the host to the new/different variable antigen types leads to elevated gamma globulins, particularly the IgM levels, including the CSF. Generally, if an individual does not have an elevated IgM, they almost certainly do not have African trypanosomiasis.
Key Points - Laboratory Diagnosis
References:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.