

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A laboratory technologist was performing a routine urinalysis microscopic examination. She saw several images that she thought were “real” but was unable to identify the structures. The presumption was that the structures were similar to some types of protozoa.


What additional information would you like to have at this point?
Are there any parasites that you think might fit the morphology seen in the images?
Scroll Down for Answer and Discussion
The images presented in Diagnostic Quiz #89 are the following:
The objects shown in this case were identified as Schistosoma haematobium eggs that had prematurely hatched in the urine, releasing the miracidia larvae. Thus, the two structures are the egg shells (upper) and the miracidium larva (lower) that has been released from the shell. The urine may have been
diluted with water or was not very concentrated (very pale and having very little debris in the sediment). The eggs had hatched prematurely. However, if the morphology is carefully examined, one can see the typical egg shell with the terminal spine, as well as the miracidia larvae released from the shell.
Note that the larvae appear enlarged when they are released from the shell

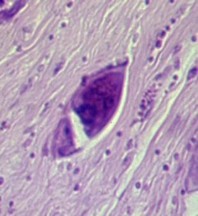
The egg on the left shows the typical terminal spine at the bottom of the egg shell; the egg in the center is an H&E preparation of an egg in tissue; the image on the right shows many eggs within a bladder biopsy.
Light infections with urinary schistosomiasis usually produce no symptoms; however, in early disease there may be dysuria and hematuria due to cystitis from deposited eggs. Depending on the worm burden, symptoms may include dysuria, frequency, and terminal or total hematuria. Hematuria is so common that in some areas of endemic infection this phenomenon was considered
to be analogous to menarche in girls (63). Symptoms are usually not seen for 3 to 6 months and may take a year or more to develop. Physical examination is usually normal, but urinalysis may reveal many red blood cells and a few white blood cells on microscopic examination; reagent strip results may indicate hematuria and proteinuria. Chronic disease may lead to major problems, including obstructive uropathy, chronic bacteriuria, bladder carcinoma, and bladder calcification.
Eggs are most highly concentrated in the tissues of the bladder and lower ureter. As the eggs become trapped in the tissues, granulomas and pseudoabscesses form, leading to fibrosis and ulceration. With extensive fibrosis, the bladder loses its contractility. The urethra frequently is occluded because of hyperplasia, polyp formation, and discharge of purulent debris
plugs from the bladder. The ureters are also frequently involved, and obstruction can cause urine reflux, hydronephrosis, retrograde infections, and renal failure. Heavy infections in males may involve the penis, resulting in elephantiasis due to blockage of the scrotal lymphatics by egg deposition.
Detection of S. haematobium eggs in 43% of semen samples with increased levels of eosinophil cationic protein suggests that the male genital organs are frequently affected.
Female genital schistosomiasis (FGS) is often associated with eggs in the cervix, vagina, and/or vulva, as seen during examination of a wet cervical biopsy specimen crushed between two glass slides. There is significant correlation between the size of the genital lesions and the number of eggs per square millimeter of crushed tissue. Women with FGS also tend to have more tumors in the vulva than do women with schistosomiasis limited to the urinary tract. In one study, only 43% of the patients with FGS had hematuria.
Carcinoma of the bladder has been frequently noted in patients infected with
S. haematobium. Many factors have been suggested as agents promoting schistosome-associated bladder cancer. N-Nitroso compounds in association with secondary bacterial infections of the urinary tract may contribute to the high prevalence of bladder cancer. Bladder cancer is the most prevalent cancer in Egyptians.
Remember that these structures are considerably larger than urinary system protozoa (Example: Trichomonas vaginalis). The S. haematobium eggs measure 112-170 by 40-70 microns, while protozoa are generally no larger than 20 microns.
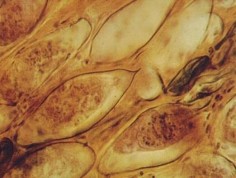
The miracidia larvae can be stained and appear in the image below:

Garcia, LS, 2016. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, DC.
Garcia, LS, 2021. Practical Guide to Diagnostic Parasitology, 3rd Ed., ASM Press, Washington, DC.
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.