

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 36 year old male from Columbia was admitted to the hospital with seizures. This patient had previously experienced convulsions when he was 13 (residual left-sided headache), but had remained asymptomatic until approximately 2 years prior to admission. The seizures had become more numerous and now occurred about once a month. The patient had experienced an inability to talk and had become unconscious for several minutes during these episodes. He had also complained of double vision. In some cases during which the patient was conscious, he was unable to talk.
On admission, the patient appeared to have partial paralysis on the left side and complained of progressive weakness, again on the left side. Computed tomographic (CT) and magnetic resonance imaging (MRI) studies revealed several intracerebral lesions, some of which appeared to be calcified. The patient underwent craniotomy, and the following structures were seen and removed. The patient had several seizures
post-surgery.
Gross specimen, measuring 3 by 4 cm.
Three cysts were removed. Routine pathology preparations revealed the following:


Images courtesy of A Pictorial Presentation of Parasites: A cooperative collection prepared and/or edited by H. Zaiman)
What organisms might be present in the images shown above?
What did the patient ingest in order to become infected?
In individuals from Mexico, Central, and South America, this parasite should be suspected in patients who present with what symptoms?
Scroll Down for Answer and Discussion
The images presented in Diagnostic Quiz #85 are the following:
The gross specimen is a Taenia solium cysticercus that has been removed from the brain.
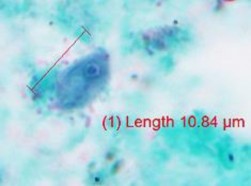
The tissue section on the left is a Taenia solium cysticercus that consists of a fluid-filled bladder containing a single protoscolex. Each cysticercus measures approximately 5 to 15 mm long by 4 to 12 mm wide (although some may be somewhat smaller). A convoluted spiral canal leads to the rostellum, and the parenchyma usually contains calcareous corpuscles.
The image on the right is a tissue section of a Taenia solium cysticercus in the brain, surrounded by fibrous tissue. The invaginated scolex is present; however, the four suckers and hooklets may not always be visible.
Parasites that come to mind include Taenia solium (pork tapeworm -cysticercosis) or Echinococcus granulosus (sheep/sheep dog tapeworm - hydatid disease).
The patient must have ingested some viable eggs of T. solium. The eggs hatch, and the larvae migrate into the body tissues. When the larvae die, they calcify and are visible radiographically. Viable cysts can be visualized using various scan methods or MRI techniques (lesions in the brain).
In patients from these geographic areas, any patient who presents with seizures should be considered for possible cysticercosis.
Comments on the Patient: This case represents an infection with Taenia solium, the cause of cysticercosis. When these larvae are found in the brain, symptoms can result from actual larval invasion of the brain tissue and/or death or the organism, which stimulates tissue reactions the larvae. It has been recommended that in every case of epilepsy occurring in a patient with no family history of seizures and no previous history of seizures in childhood, the probability of cysticercosis should be considered. Other symptoms, including abnormal behavior, transient paresis, intermittent obstructive hydrocephalus, disequilibrium meningoencephalitis, and visual problems, may also be present. In this patient there was a history of seizures in childhood, and many of the key symptoms of cysticercosis were also present.
Comments on the Organism: The cysticercus is an ovoid, milky white bladder with the head invaginated into the bladder. The bladder worms measure 5 mm long by 8 to 10 mm wide, except in brain or subminingeal spaces where they can have a volume of about 60 ml. The larval forms of T. solium (cysticerci) have been recovered from all areas of the body, and symptoms depend on the body site involved. The presence of cysticerci in the brain represents the most frequent parasitic infection of the human nervous system and the most common cause of adult-onset epilepsy throughout the world.
On ingestion by hogs or humans, the eggs of T. solium hatch in the duodenum or jejunum after exposure to gastric juice in the stomach. The released oncospheres penetrate the intestinal wall, are carried via the mesenteric venules throughout the body, and are filtered out in the subcutaneous and intramuscular tissues, the eyes, the brain, and other body sites. Neurocysticercosis usually affects males and females of all ages, with a peak incidence between 30 and 50 years of age.
Taenia solium Key Points - Laboratory Diagnosis
Identification of the adult worms to the species level (T. solium or T. saginata) is not possible from the eggs, since the eggs from both species look identical (see below).
Identification is usually based on examination of the gravid proglottids (see below) after India ink injection staining or some other clearing mechanism. The main lateral uterine branches are counted and T. solium has 7 to 13 branches, while T. saginata has 15 to 20 branches (counted on one side only where the lateral branches come off the main stem). NOTE: Because of the possible danger of egg ingestion, specimens and proglottids should be handled with extreme care. The proglottid uterine structure will be packed with viable, infectious eggs.
If the scolex is found, there are four suckers and an armed rostellum with hooks (see below).
The diagnosis of cysticercosis usually depends on surgical removal of the parasite and microscopic examination for the presence of suckers and hooks on the scolex. Routine histology can also be performed.
Multiple larvae are frequently present, and the presence of cysticerci in the subcutaneous or muscle tissues indicates that the brain is probably also involved.
If the racemose form is present in the brain, the CT scan will not be able to distinguish the lesion from that caused by other tumors.
Although serologic testing is helpful in some cases, there may be cross-reactivity between cysticercosis and hydatid infection (Echinococcus spp.), and the results may be erratic. The immunoblot for neurocysticercosis provides a much improved test, with a sensitivity of 98% and a specificity of 100%. The enzyme-linked immunoelectrotransfer blot (EITB) assay using blood dried on filter paper has proven to be a convenient, economical way of handling field samples, particularly in underdeveloped countries. There is no decrease in sensitivity compared with traditional serum samples used in the EITB.


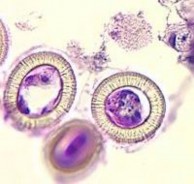
Taenia spp. eggs containing six-hooked oncosphere: note the striated shell; image on the right stained with H&E – striations visible, but internal hooklets not clear.
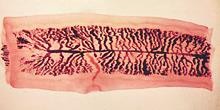

Taenia saginata (beef tapeworm) and Taenia solium (pork tapeworm) gravid proglottids: note the number of branches
Garcia, L.S. 2016. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.
Meyers, W.M. (ed). 2000. Pathology of Infectious Diseases, Vol 1, Helminthiases, Armed Forces Institute of Pathology, American Registry of Pathology, Washington, DC.
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.