Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
The patient was a 53 year old male, HIV negative, who was previously treated for tuberculosis several years before. He presented with weight loss, cough with purulent expectoration, and pulmonary fibrosis. Stains of sputum specimens were negative for acid-fast bacilli; however, pink structures were seen that were unidentified.
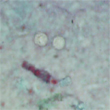
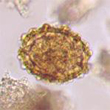
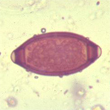
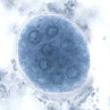
In a routine stool examination for ova and parasites, the following image was seen on the trichrome stain. Other organisms seen in the concentration sediment examination are also seen below:
|
These two structures on the trichrome permanent stained slide failed to stain and measured approximately 9 microns in diameter. They appeared to have no internal structure.
|
|
|
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #51
The images presented in Diagnostic Quiz #51 are the following:
Comment:
In Cyclospora infections, there is generally 1 day of malaise and low-grade fever, with rapid onset of diarrhea of up to seven stools per day. There may also be fatigue, anorexia, vomiting, myalgia, and weight loss with remission of self-limiting diarrhea in 3 to 4 days, followed by relapses lasting from 4 to 7 weeks. In patients with AIDS, symptoms may persist for as long as 12 weeks; biliary disease has also been reported in this group. Diarrhea alternating with constipation has also been reported; this is not uncommon in a number of protozoal gastrointestinal infections. The majority of infected individuals have intermittent diarrhea for 2 to 3 weeks, and many complained of intense fatigue, as well as anorexia and myalgia, during the illness. The clinical presentation of patients infected with this organism is similar to that of patients infected with Cryptosporidium spp.
It is highly unusual to see this organism in sputum, and reports of such findings are very rare. It is suspected that the patient may have come in contact with either several potential sources of infection or may have acquired a large infective dose of oocysts as a single exposure.
The transmission of Cyclospora is thought to be fecal-oral, although direct person-to-person transmission has not be well documented and may not be a factor since sporulation takes a number of days. Outbreaks linked to contaminated water and various types of fresh produce (raspberries, basil, baby lettuce leaves, and snow peas) have been reported.
Life Cycle:
Unsporulated oocysts are passed in the stool and sporulation occurs within approximately 5 to 13 days. In patients who are found to have Cyclospora in their stool specimens, parasites with coccidian characteristics have been found within the jejunal enterocytes. Complete sporulation produces two sporocysts that rupture to reveal two crescent-shaped sporozoites measuring 1.2 by 9.0 μm.
Diagnosis:
In clean wet mounts, the organisms are seen as nonrefractile spheres and are acid-fast variable with the modified acid-fast stain; those that are unstained appear as glassy, wrinkled spheres. Modified acid-fast stains stain the oocysts from light pink to deep red, some of which will contain granules or have a bubbly appearance. It is very important to be aware of these organisms when the modified acid-fast stain is used for Cryptosporidium spp. and other similar but larger structures (approximately twice the size of Cryptosporidium oocysts) are seen in the stained smear. The acid decolorizer should be no stronger than 1-3% sulfuric acid; use of a stronger decolorizer may remove too much stain from the Cyclospora oocysts. It is important for laboratories to measure all acid-fast oocysts, particularly if they appear to be somewhat larger than those of Cryptosporidium. Under epifluorescence, the oocysts autofluoresce strong green (450 to 490 DM excitation filter) or intense blue (365 DM excitation filter). It is strongly recommended that during concentration (formalin/ethyl-acetate) of stool specimens, the centrifugation time and speed should be 10 minutes at 500 x g.
Using a modified safranin technique, the oocysts uniformly stain a brilliant reddish orange if fecal smears are heated in a microwave during staining. The stained slide can also be examined using epifluorescence microscopy first, and suspect oocysts can be confirmed using brightfield microscopy.
Epidemiology and Control:
Published reports indicate that individuals of all ages, including those who are immunocompetent and immunosuppressed, can become infected. In Peru, infections with this Cyclospora have shown some seasonal variation, with peaks during the April-to-June time frame. This pattern is similar to that seen in Peru in Cryptosporidium infections. Preliminary data and extrapolation from what we currently know about cryptosporidiosis suggest that modes of transmission may be similar, particularly considering waterborne transmission. Certainly it is recommended that fresh produce be thoroughly washed prior to ingestion.
Cyclospora cayetanensis Key Points--Laboratory Diagnosis
Remember: do not use a strong decolorizer; a 1-3% sulfuric acid is recommended and will also work well for modified acid-fast stains for Cryptosporidium spp. and/or Isospora (Cystoisospora) belli. The original 3-5% sulfuric acid is usually too strong for Cyclospora and removes too much color. Even with the 1% acid decolorizer, some oocysts may appear clear or very pale. Most laboratories are currently using 1% acid for the decolorizer.
Treatment: Trimethroprim-sulfamethoxazole (TMP-SMX) is currently the drug of choice; relief of symptoms has been seen in 1 to 3 days posttreatment. However, recurrence of symptoms can occur within 1 to 3 months posttreatment in over 40% of the patients. In a study using TMP-SMX in Nepal, shedding of oocysts and symptoms disappeared after 7 days of treatment.
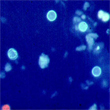
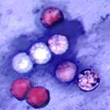
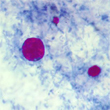
|
|
|
Three images of Cyclospora cayetanensis oocysts from a positive stool specimen (from left to right: autofluorescence using Calcofluor filters; modified acid-fast stain; modified acid-fast stain showing Cyclospora [large], Cryptosporidium [medium], and a pink artifact [small]). Note the oocysts in the modified acid-fast stain range from clear to dark pink to red or even purple. The oocysts are often described as looking like "wrinkled cellophane" and measure 8 to 10 microns. Cryptosporidium oocysts measure 4 to 6 microns; sporozoites can often be seen in these oocysts, while Cyclospora oocysts are not sporulated when passed. Regardless of whether or not you see sporozoites within the oocyst wall, Cryptosporidium oocysts are immediately infectious, while those of Cyclospora are not.
References:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.