Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 37 year old male was admitted to the hospital with complaints of severe diarrhea that had become worse over a period of about two weeks. This patient had previously been diagnosed as having AIDS and had been hospitalized several times for pneumonia. This case was seen in 1993.
He was treated with supportive care, and various specimens were submitted for diagnostic testing. Based on the image below, what do you think the diagnosis should be? What infection most likely matches this image?
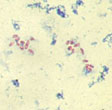
Modified acid-fast stain
Based on this finding, additional testing was performed and the following images were seen.
|
|
|
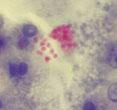
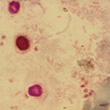
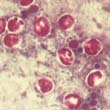
(Left - 2) Ryan-Blue modified trichrome; (Center - 3) Ryan-Blue modified trichrome (urine sediment); (Right - 4) combination modified acid-fast/modified trichrome
What organisms might be present in these images shown above?
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #28
The images presented in Diagnostic Quiz #28 are the following:
Comments on the Patient: This case represents a dual infection with Cryptosporidium spp and microsporidia in an AIDS patient. In a compromised patient, the diarrhea can be quite severe and prolonged, with tremendous fluid loss and eventual death. With the advent of the use of Highly Active Antiretroviral Therapy (HAART) (from 1996 on), there has been a significant reduction in the incidence of cryptosporidiosis in this patient population. Unfortunately, this patient was seen prior to the introduction of HAART.
Comments on the Organisms: Cryptosporidium is worldwide in distribution, and although the first cases in the literature indicated the patients were immunosuppressed or immunodeficient, much of the published literature reports infections in patients with a normal immune capability. In patients with a normal immune capability, cryptosporidiosis is self-limiting. However, in certain compromised patients, the diarrhea can be very severe and prolonged, with eventual death as the outcome. Clinical symptoms include nausea, low-grade fever, abdominal cramps, anorexia, and 5 to 10 watery stools per day. Fluid loss in these patients is significant and has been reported to be as great as 17 liters/day. Although many therapeutic regimens have been tried, there is no completely satisfactory therapy for cryptosporidiosis in humans. Respiratory cryptosporidiosis has also been reported in AIDS patients. Sputum specimens should be submitted in 10% formalin or as a fresh specimen and can be examined by using the same techniques as used for stool samples.
Cryptosporidium spp. Key Points--Laboratory Diagnosis
The microsporidia are obligate intracellular parasites that have been recognized in a variety of animals, particularly invertebrates; the organisms found in humans tend to be quite small, ranging from 1.5 to 2 microns. Until recently, awareness and understanding of human infections have been marginal; only with increased understanding of AIDS within the immunosuppressed population has attention been focused on these organisms. Limited availability of EM capability has also played a role in our inability to recognize and diagnose these infections. Current genera include: Brachiola spp., Encephalitozoon spp., Septata spp., Enterocytozoon spp., Microsporidium spp., Nosema spp., Pleistophora spp., Trachipleistophora spp., Anncaliia, and Vittaforma spp.
A number of cases of infection with Enterocytozoon bieneusi and/or Encephalitozoon (Septata) intestinalis have been reported in AIDS patients. Chronic intractable diarrhea, fever, malaise, and weight loss are symptoms with E. bieneusi infections, symptoms that are similar to those seen with cryptosporidiosis or isosporiasis. These patients have already been diagnosed with AIDS and each day tend to have four to eight watery, nonbloody stools which can be accompanied by nausea and anorexia. There may be dehydration with mild hypokalemia and hypomagnesia, as well as d-xylose and fat malabsorption. The patients tend to be severely immunodeficient, with a CD4 count always below 200 and often below 100. E. bieneusi infection has also been implicated in AIDS-related sclerosing cholangitis. Dissemination to kidneys, lower airways and biliary tract appears to occur via infected macrophages. Infections with E. intestinalis tend to respond to therapy with albendazole, unlike the infections with E. bieneusi.
E. bieneusi spores have been identified in the sputum and bronchoalveolar lavage, as well as stool samples, from a patient with a 2-year history of intestinal microsporidiosis. Although no pulmonary pathology could be established in this or one other reported case, it is well established that E. bieneusi is capable of colonizing the respiratory tract and these clinical specimens may reveal the presence of spores. Using transmission electron microscopy, multiorgan microsporidiosis due to E. bieneusi has been diagnosed in an HIV-infected patient; organisms were recovered in stools, duodenal biopsy, nasal discharge, and sputum. Infection with this organism has also been reported in individuals with intact immune function; symptoms were self-limited and diarrheal disease resolved within 2 weeks; a number of other cases have been reported in immunocompetent people. These cases suggest that E. bieneusi may be more commonly associated with sporadic diarrheal disease than was suspected and that the immune system may play a role in the control of this organism within the intestine.
Microsporidia Key Points - Laboratory Diagnosis
References
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.