Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 70-year-old man presented to his physician with a lesion on his arm. About 6 weeks prior, he had noticed a small, red area on his arm. There was some itching and over the next few weeks, the area ulcerated and measured about an inch in diameter. There was no drainage. He indicated he was feeling well and had not had any fever, chills, anorexia, or weight loss. His medical history was unremarkable.
The ulcer has a moist base and raised borders as seen below:

The lesion measured about 1 inch in diameter, and was moist with raised borders. There was no drainage; however, the lesion did appear to be infected.
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #15
The images presented in Diagnostic Quiz #15 are the following:
Comment: This is a case of a man who had cutaneous leishmaniasis.
|
|
|
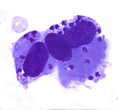
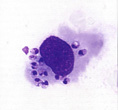
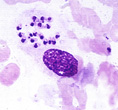
Three examples of Leishmania spp. amastigotes from a skin ulcer. Note each amastigote contains a nucleus and the bar-shaped kinetoplast. These preparations have been stained with a blood stain.
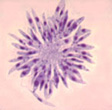
These promastigotes are obtained from a culture in which you can see the bar-shaped kinetoplast in the organism closest to the center of the group "rosette" - aspirates of skin can be inoculated into several media for the confirmation of leishmaniasis. The preparation has also been stained using a blood stain.
Note: it is important to remember that with cutaneous and/or mucocutaneous lesions, the only area where the parasites will be found is the lesion itself. Unless the infection is the visceral type (L. donovani), no organisms will be found in the spleen, bone marrow and/or liver. There may be exceptions in cutaneous or mucocutaneous types of disease in which the amastigotes are found in other parts of the reticuloendothelial system; however, this tends to be unusual.
New World cutaneous leishmaniasis extends from southern Texas and Arizona to Latin and South America and the Caribbean islands. As seen in Old World leishmaniasis, there is a wide range of disease presentation and separation based on clinical signs and symptoms is not possible. Organisms in this group belong to the subgenera Leishmania and Viannia. Within the subgenus Leishmania is the L. mexicana complex, and within the Viannia subgenus are the L. braziliensis complex and the L. guyanensis complex. It is very likely that taxonomy will continue to change as molecular methods reveal genetic differences and similarities among the various genera and species. Common names for New World CL include uta (Peru), dicera de Baurid (Brazil), chiclero ulcer or bay sore (Mexico), and pian bois or forest yaws (Guyana). Collectively, this group has also been called American CL. This disease is quite old and has even been depicted on pottery from Peru and Ecuador that has been dated c. AD 400-900.
The lesions of New World CL are very similar to those seen with Old World cutaneous disease. Weeks to months after infection, an erythematous, often pruritic papule develops at the bite site. This papule may become scaly and enlarge, developing a central ulcer surrounded by a raised margin. Disease progression at this point will vary, depending on the species involved. Lesions may be single or multiple and usually occur on exposed areas of the body. Many lesions may self-heal over a time frame of approximately 6 months; however, lesions on the ear occur in 40% of the patients and are chronic, lasting many years. Ulcerations on the ears may be quite destructive, but cause the patient few problems. L. mexicana lesions are usually single, self-limiting cutaneous papules, nodules or ulcers that are painless and are found on the face and ears. Other infections that are usually associated with single cutaneous lesions include L. colombiensis, L. amazonensis, L. garnhami, L. lainsoni, L. peruviana, and L. venezuelensis. Multiple lesions due to spread along lymphatics are common with L. guyanensis infections and subcutaneous lymphatic nodules can be seen with L. panamensis; the lesions can mimic those seen in sporotrichosis. New World CL will have to be distinguished from sporotrichosis, blastomycosis, yaws, syphilis, cutaneous tuberculosis, Mycobacterium marinum infection, and dermatologic cancers.
In areas of the world where physicians are very familiar with leishmaniasis, the diagnosis may be made on clinical grounds. However, in other areas of the world where the disease is rare, the condition may not be recognized as leishmaniasis. Definitive diagnosis depends on demonstrating the amastigotes in tissue specimens or the promastigotes in culture. Newer results suggest that PCR is a valuable tool for the diagnosis of leishmaniasis on a routine basis and can provide valuable epidemiological information in endemic areas. Cutaneous leishmaniasis may have to be differentiated from a number of other lesions and diseases, including basal cell carcinoma, tuberculosis, various mycoses, cheloid and lepromatous leprosy.
The ability to detect parasites in aspirates, scrapings or biopsy specimens will depend on the number of amastigotes present, the level of the host immune response, the absence or presence of bacterial and/or fungal contamination within the lesion, and whether the specimen is collected from an active or healing lesion. If the patient has multiple lesions, specimens should be collected from the more recent or active lesions. These lesions should be thoroughly cleaned with 70% alcohol and necrotic debris should be removed to prevent the risk of bacterial and/or fungal contamination of the specimen. Also, the specimen should be taken from the advancing margin of the lesion; the central portion of the ulcer will contain nothing but necrotic debris.
The specimen of choice would be a collection of several punch biopsy specimens, taken from the most active lesion areas. Biopsy specimens can be divided and used for cultures and touch preparations; some material should always be saved and submitted for routine histology. The biopsy specimen can be used to make impression smears (touch preparations); these smears should be prepared after portions of the specimen have been placed in culture media using sterile technique. After cleaning off any excess blood, make a horizontal cut through the biopsy core and gently touch the cut surface to glass slides; remember to prepare multiple slides. Once material has been set up for culture and touch preparations have been made, the remainder of the tissue can then be sent to pathology for routine processing.
Culture media that has been used for the recovery and growth of the leishmaniae include Novy, MacNeal and Nicolle's medium and Schneider's Drosophila medium supplemented with 30% fetal bovine serum. Patient cultures should not be set unless the laboratory maintains specific organism strains for quality control checks. Both the control and patient cultures should be examined twice weekly for the first 2 weeks and once a week thereafter for up to 4 weeks before they are called negative. Promastigote stages can be detected microscopically in wet mounts taken from centrifuges culture fluid. This material can also be stained with a blood stain to facilitate observation at a higher magnification.
In contrast to Old World CL, systemic chemotherapy is recommended for New World CL. Differences between the two types of CL tend to justify this recommendation and include cases with multiple lesions; the long-term, chronic nature of some infections; and the tendency for disease progression and mucosal involvement in the absence of chemotherapy.
References:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.