

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
Presentation of Quiz #71
The patient is a 65-year-old female who presented with a right upper lung mass. She had been diagnosed with cervical cancer approximately 8 years ago and was successfully treated. The following image/structure was seen in a bronchial washing. The presumptive identification was “ciliate protozoa” identification to species unknown, but probably something similar to Balantidium coli or some type of free-living protozoan contaminant. When seen in wet preparations prior to fixation or staining, the motility was evident.

Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #71
An additional specimen revealed the following image from a cluster of bronchial epithelial cells, a feature of benign bronchial epithelium.
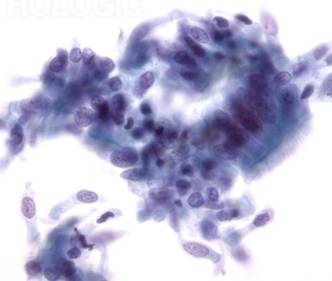
Using morphologic criteria and routine staining (Diff-Quik rapid stain), the cells were identified as ciliated epithelial cells, rather than ciliated protozoa. In both images, the cilia can clearly be seen. Thus, based on these criteria, ciliocytophthoria can be differentiated from a true ciliated protozoan pathogen (Balantidium coli) or free-living protozoa as contaminant artifacts.
Discussion:
Detached ciliary tufts (ciliocytophthoria) have been seen in a variety of body fluids (especially peritoneal and amniotic fluids; also respiratory specimens). These tufts are the remnants of ciliated epithelium that are found as a part of normal cellular turnover in a number of sites: respiratory tract and sinuses, ventricles of the brain, central canal of the spinal cord, and epithelia of the male and female reproductive tracts. The tufts are motile, measure 10 to 15 µm in diameter, and can be confused with ciliated or flagellated protozoa. However, when they are carefully examined on a stained smear, there is no internal structure like that seen in protozoa (1-4). Ciliocytophthoria are anucleate remnants of these ciliated cells. However, in some cases, the cell nuclei are clearly visible. The ciliated tufts can be seen on the cells in the figure above.
These cells have been found in many clinical specimens, including peritoneal fluid. Recognition of these uncommon structures can be important in avoiding a misdiagnosis with a suspect protozoan infection. This has also been recognized as a potential problem in the virology laboratory. The difference between ciliocytophthoria and ciliated or flagellated parasites becomes very important during examination of specimens submitted for cytologic testing. Also in performing immunofluorescence assays (DFAs) used in the virology laboratory for the rapid detection of viruses, assessment of the cellularity of specimens is required for the most effective use of the DFA assay.
References:
1.Garcia, LS, 2016. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, DC.
2. Khan, S, VA Kumar, A Venkitachalam, V Vishwam, K Dinesh, S Karim. 2015. Detached ciliary tufts masquerading as free-living amoebae. Int J Infect Dis 30:142-143.
3. Vila, M, K Thompson, G Erdem. 2011. Motile ciliary microorganisms in peritoneal fluid. Diagn Cytopathol 39:606-607.
4. Hadziyannis, E, B Yen-Lieberman, G Hall, GW Procop. 2000. Ciliocytophthoria in clinical virology. Arch Pathol Lab Med 124:1220-1223.
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.