Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 64-year-old male presented to his physician with a history of symptoms, beginning about 10 days before. Symptoms included general malaise, followed by fever, shaking chills, profuse sweating, arthralgias, myalgias, fatigue, and weakness. The man lived in eastern Long Island and owned property which had not yet been developed. He, his wife, and three dogs went hiking on the property quite often.
Although both the man and his wife were aware of the presence of deer ticks, Ixodes scapularis, on the property, neither could remember seeing any ticks or being bitten. On presentation to the physician, initial tests did not confirm any particular infection or illness. Hepatosplenomegaly was present and the patient had slightly elevated bilirubin and transaminase levels as a result of hemolytic anemia.
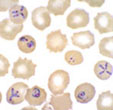
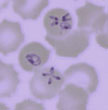
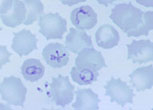
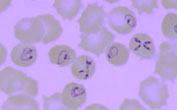
Blood film examinations were initially negative; however, after an additional 5 days, the following images were seen during microscopic review of thin blood films.
Please comment on the possible diagnosis.
1. Thin blood film |
2. Thin blood film |
3. Thin blood film |
4. Thin blood film |
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #8
The images presented in Diagnostic Quiz #8 are the following:
Comment: The patient had a Babesia microti infection transmitted by the bite of the deer tick, Ixodes scapularis. The parasites appear as pleomorphic, ring like structures. They can resemble the early forms of malarial parasites, particularly P. falciparum. In figure 3 above, you can see the rings outside of the RBCs; this rarely occurs in a case of P. falciparum malaria. However, you can see there are many similarities between the Babesia ring like structures and the rings of P. falciparum However, the Babesia parasites tend to be much more pleomorphic than those of malaria. Also, in cases of babesiosis, there may be five or six rings per cell, while in a case of P. falciparum malaria, generally two rings per cell tends to be more the case. An exception would be the photograph on the right (below) where four malaria rings can be seen in a single RBC.


Plasmodium falciparum rings (young trophozoites)
Comments:
Potential diagnostic problems with the use of automated differential instruments have been reported; however, in this case the parasitemia may have been too low when the patient first presented to the physician to be detected by automation and/or routine thin blood film examination. Unless the patient has been splenectomized or is immunocompromised for some other reason, most patients tend to have a low parasitemia. Thus, both thick and thin blood films stained with Giemsa stain (or some other appropriate blood stain) must be examined. When the organisms cannot be demonstrated in a suspected patient, blood can be inoculated intraperitoneally into a hamster or gerbil. However, not all Babesia species will infect these animals. However, in many cases, the organisms can be demonstrated within a few days, with the same parasite morphology as that seen in humans.
Often, babesiosis can be managed with supportive care. Currently, the combination of clindamycin plus quinine has been recommended as the standard treatment regimen. However, failure to eliminate the infection in some immunocompromised patients has been reported. The use of azithromycin in combination with quinine may be considered as an alternative therapy.
Although many infections seen in the northeastern United States are subclinical, infections in California and Europe tend to present as a fulminant, febrile, hemolytic disease affecting splenectomized or immunosuppressed individuals. Any person with babesiosis acquired in Europe should be treated on an emergency basis. They should receive prompt specific therapy to reduce parasitemia and to prevent extensive hemolysis and potential renal failure. A rapidly increasing parasitemia characterized by infections with B. divergens may require massive exchange transfusion. With the onset of hemoglobinuria, rapidly increasing intravascular hemolysis leads to renal failure.
Prevention depends on the avoidance of ticks or their prompt removal once detected. Apparently, there are no fully effective tick repellents. If symptoms appear 1 to 2 weeks after a tick bite, a physician should be consulted. It is also well established that under blood banking conditions (4C for 30 days), B. microti can remain infective and that transfusion-acquired infection with this parasite could occur during the normal storage time for blood.
The most common approach used to protect humans from infection involves methods to reduce the tick density, including spraying of vegetation. Repellents can be helpful for personal protection; however, daily examination of the body surface of a person who may have come in contact with ticks is critical. If ticks are found, they should be removed immediately to take advantage of the lag time between attachment to the human and transmission of the infection (usually 50 to 60 hours).
Key Points - Laboratory Diagnosis
References
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.