Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 4-year-old female was taken to her physician with a continuing history of symptoms, including irritability, poor sleeping patterns, anal irritation, and vague abdominal complaints, including diarrhea. Her mother reported the child had bouts of diarrhea, with two or three movements per day, and her daughter "just didn't feel very good". Three stool specimens had been submitted for examination and were reported as negative. The patient improved somewhat and no further testing was performed.
About 10 days later, the patient reported another bout with diarrhea and was seen by a relative who was a physician. Additional stool examinations were ordered and the patient was diagnosed with two parasitic infections.
Please comment on the possible diagnosis related to the history, the patient's clinical symptoms and the laboratory test results to date. Examination of the stools and an anal impression cellulose tape revealed the following:
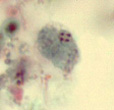
1. Trichrome stain of fecal specimen |
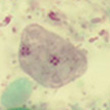
2. Trichrome stain of fecal specimen |
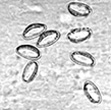
3. Anal impression: cellulose tape |
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #11
The images presented in Diagnostic Quiz #11 are the following:
Comment: This is a case of a young child who was infected with Dientamoeba fragilis and pinworm (Enterobius vermicularis). Since the first set of fecal examinations were negative, it would be important to find out whether the laboratory included the permanent stained smear as a routine part of the O & P examination. If not, it is very likely that an infection with D. fragilis would be missed (trophozoite only, cyst form very rare in clinical specimens).
Dientamoeba fragilis
The life cycle and mode of transmission for D. fragilis have recently been clarified. Transmission via helminth eggs (Ascaris and Enterobius) has been postulated. The cyst stage has been confirmed; transmission is quite probably via the cyst form, as well. The trophozoite is characterized as having one (20 to 40%) or two (60 to 80%) nuclei. The nuclear chromatin is usually fragmented into three to five granules, and there is normally no peripheral chromatin on the nuclear membrane. The cyst form is rarely seen (about 1% in any clinical specimen; two fragmented nuclei and distinct cyst wall), thus the identification relies primarily on the trophozoite form.
In some organisms, the nuclear chromatin may tend to mimic that of Endolimax nana, Entamoeba hartmanni, or even Chilomastix mesnili, particularly if the organisms are overstained. The cytoplasm is usually vacuolated and may contain ingested debris as well as some large, uniform granules. The cytoplasm can also appear uniform and clean with few inclusions. There can also be considerable size and shape variation among organisms, even on a single smear.
D. fragilis has been associated with a wide range of symptoms. Case reports of children infected with D. fragilis reveal a number of symptoms, including intermittent diarrhea, abdominal pain, nausea, anorexia, malaise, fatigue, poor weight gain, and unexplained eosinophilia. The most common symptoms in patients infected with this parasite appear to be intermittent diarrhea and fatigue. In some patients, both the organism and the symptoms may persist or reappear until appropriate treatment is initiated.
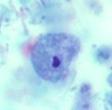
Diagnosis of D. fragilis infections depends on proper collection and processing techniques (a minimum of three fecal specimens). Although survival time for this parasite has been reported as 24 to 48 h, the survival time in terms of morphology is limited, and stool specimens must be examined immediately or preserved in a suitable fixative soon after defecation. It is particularly important that permanent stained smears of stool material be examined with an oil immersion lens (1,000 x). These organisms have been recovered in formed stool; thus, a permanent stained smear must be prepared for every stool submitted for a parasite examination. The organisms will rarely be seen in a wet preparation. Note in the image below that the organism resembles E. nana, but one can see "clearing" in the center of the karyosome; this indicates the nuclear material is beginning to fragment into the chromatin dots more commonly seen in the D. fragilis nucleus.
Dientamoeba fragilis trophozoite: karyosome beginning to fragment |
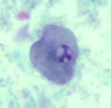
Endolimax nana trophozoite |
Endolimax nana trophozoite |
Entamoeba hartmanni trophozoite |
Enterobius vermicularis (pinworm)
E. vermicularis is thought to cause the world's most common human parasitic infection. It has been said, ``You had this infection as a child; you have it now; or you will get it again when you have children!'' The infection is more prevalent in the cool and temperate zones where people tend to bathe less often and change their underclothes less frequently. Prevalence in children can be high, a fact that has been recorded despite the difficulties in confirming the infection.
The female worm measures 8 to 13 mm long by 0.3 to 0.5 mm wide and has a pointed tail (thus the name pinworm). The male is much smaller, measuring 2 to 5 mm long by 0.1 to 0.2 mm wide, and has a curved caudal end. Infection in humans is initiated by the ingestion of infective eggs which hatch in the intestine (cecal region), where they develop into the adult worms. It probably takes about 1 month for the female to mature and begin egg production.
After fertilization of the female worms, the males usually die and may be passed out in the stool. In gravid females, almost the entire body is filled with eggs. At this point, the female migrates down the colon and out the anus, where the eggs are deposited on the perianal and perineal skin. Occasionally the female worm may migrate into the vagina. It is speculated that after egg deposition, the female worm returns to the intestine; however, this has not been proven.
Occasionally when the bolus of stool passes out of the anus, adult worms become attached to the stool and can be found on the surface. Adult worms can also sometimes be picked up on the Scotch tape preparations used to diagnose this infection. Although egg deposition usually does not occur in the intestine, some eggs may be recovered in the stool. The eggs are fully embryonated and infective within a few hours. The eggs have been described as footballs with one side flattened. They are oval, compressed laterally, and flattened on one side and measure 50 to 60 µm long by 20 to 30 µm wide.
The most striking symptom of this infection is pruritus, which is caused by the migration of the female worms from the anus onto the perianal skin before egg deposition. The sometimes intense itching results in scratching and occasional scarification. In most infected people, this may be the only symptom, and many individuals may remain asymptomatic. Eosinophilia may or may not be present. Although tissue invasion has been attributed to the pinworm, these cases are not numerous.
Infections tend to be more common in children and occur more often in females than in males. In heavily infected females, there may be a mucoid vaginal discharge, with subsequent migration of the worms into the vagina, uterus, or fallopian tubes, where they become encapsulated. Other symptoms have also been attributed to the pinworm infection, particularly in children; they include nervousness, insomnia, nightmares, and even convulsions.

Enterobius vermicularis adult female worms
References:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.