Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 35-year-old male with AIDS presented to his physician with a continuing history of symptoms, including chronic intractable diarrhea, fever, malaise, and weight loss. He reported having four to six watery, nonbloody stools per day, and often felt nauseated. The patient had also been diagnosed with nephritis. Three ova and parasite examinations had been performed and were reported as negative. The following laboratory tests were then ordered: modified acid-fast stains for the coccidia and modified trichrome stains for the microsporidia.
Please comment on the possible diagnosis related to the history of AIDS, the patient's clinical symptoms and the laboratory test results to date. Examination of the modified acid-fast stained smears and the modified trichrome stained smears revealed the following.
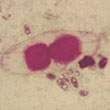
1. Modified acid-fast stain, modified trichrome stain- stool |
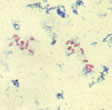
2. Modified trichrome stain (Ryan Blue) - stool |
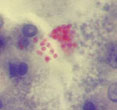
3. Modified trichrome stain (Ryan Blue) - urine |
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #10
The images presented in Diagnostic Quiz #10 are the following:
Comment: This was a case of microsporidiosis in an immunocompromised patient with AIDS. The two organisms that are found in the intestinal tract are Enterocytozoon bieneusi and Encephalitozoon (Septata) intestinalis. The spores seen in the stool and urine measure approximately 1-2 microns, and the morphology does not allow differentiation between the two genera. Both can also disseminate to the kidneys and elsewhere, so they could both be found in urine. The patient also had an infection with Isospora belli; these oocysts stained using the modified acid-fast stain, as seen above. The first photograph represents a combination stain, using both the modified acid-fast and modified trichrome staining formulas. Organisms that would stain using this method include: Cryptosporidium parvum, Cyclospora cayetanensis, Isospora belli and the microsporidia.
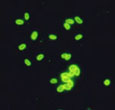
Encephalitozoon spp. (probably intestinalis) (Monoclonal reagent) |
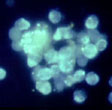
Microsporidian spores in urine (Calcofluor white) |
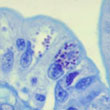
Spores in enterocytes (Giemsa stain) |
Comments:
Using an experimental monoclonal reagent directed against Encephalitozoon spp., the spores were found to fluoresce, thus confirming spores in this genus were present. Smears were also stained using the optical brightening agent, calcofluor white. Although the spores did stain, this approach is non-specific and results cannot differentiate among the different genera of microsporidia. Unfortunately, commercial immunoassay reagents are not yet available for the detection and/or differentiation of the microsporidia. One can also see the spores within the enterocytes within the intestine; this preparation was stained with Giemsa stain.
Microsporidiosis is an important emerging opportunistic infection in HIV-infected patients and appears to have an ever-expanding clinicopathologic spectrum. This infection has also been identified in transplant patients. Although the majority of information is available regarding the immunocompromised host, it is likely that the immunocompetent host can also acquire these infections; there may be many more infections seen, but not recognized, in normal individuals with diarrhea.
The spore is the only life cycle stage able to survive outside of the host cell and is the infective stage. The spore normally reaches the new host through ingestion, although other routes of infection have been identified including: inhalation, direct inoculation, and sexual transmission. Currently, there are many genera and species of microsporidia that have been implicated in human infections. There are a number of methods used for the recovery and identification of microsporidia in clinical specimens. Tissue Gram stains, PAS, silver stains, Giemsa stain or modified trichrome stains are available. Differentiation to the genus level often requires specific experimental reagents or electron microscopy. A positive infection should be reported as: Microsporidian spores seen; unable to identify to the genus level.
Key Points - Laboratory Diagnosis
References:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.