Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
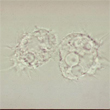
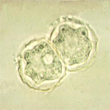
A 28 year old male presented with rhinosinusitis and was diagnosed as having a squamous cell carcinoma of the nasal septum. He was a presumptive healthy and immunocompetent individual; however, he was later diagnosed with AIDS. As the diagnostic workup was expanded and other possible etiologic agents were considered, the following images were seen from agar culture plates.
|
|
Based on these images and the patient history, answer the following questions.
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #50
Answers to Questions:
Comments on the Patient:
Although this patient was diagnosed as having a squamous cell carcinoma of the nasal septum, this was an incorrect diagnosis. Once the diagnosis of AIDS was made, the workup was expanded to include possible parasitic pathogens, particularly organisms in the free-living amebae group. The final diagnosis was AIDS along with disseminated acanthamoebiasis. STAT TESTING
This case points up the importance of considering all possibilities, particularly in a patient who appears to be immunocompetent, but who may actually be immunocompromised for one or more reasons.
Comments on Disseminated Acanthamoeba Infection:
An early diagnosis can be made if amebic infection is considered in patients with various presentations. Acanthamoeba spp. are well accepted as opportunistic pathogens in immunocompromised patients with AIDS, generally those with a low CD4+ cell count. Unfortunately, the diagnosis of this infection requires a high index of suspicion, since both clinical and histological findings may mimic those of disseminated fungal or algal disease or non-infectious causes such as carcinoma.
The primary site of infection is thought to be the sinuses and lungs. The skin is also thought to be a possible portal of entry. Clinical manifestations may include general complaints such as fever and chills, nasal congestion or lesions, neurologic symptoms, and musculoskeletal and cutaneous lesions. In patients with disseminated disease, the duration of infection from onset to death can range from 7 days to 5 months. Since early therapy can alter the clinical outcome, recognition of this disease is critical. It is important to initiate appropriate diagnostic testing for confirmation of the causative agent as soon as possible.
Comments on the Organism:
Acanthamoeba have been found in the upper respiratory tract in humans with and without symptoms. In cases of disseminated disease the portal entry remains unknown, but is suspected to be the respiratory tract. However in patients with skin lesions, the skin may be the site of primary inoculation. Although many of the reported cases have been seen in compromised patients, cases have also occurred in immunologically competent hosts. Mixed infections caused by Acanthamoeba and Naegleria (sinusitis) have been documented; these infections with free-living amebae MUST BE CONSIDERED, ESPECIALLY WHEN BACTERIA OR FUNGI ARE NOT FOUND IN GRAM STAINS (3).
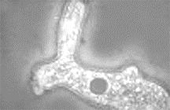
Although Naegleria dissemination outside the central nervous system may occur, it is apparently rare and unlike the protracted situation seen in this patient. The morphology of Naegleria trophozoites is quite different from Acanthamoeba and an image can be seen below. Note the lobular pseudopodia as compared with the "spiky" pseudopodia seen in Acanthamoeba trophozoites above.
|
Comments on the Culture System:
The non-nutrient agar plates are made using Page's saline. Prior to use, the plates should be removed from the refrigerator and placed at 37C for 30 min. Add about 0.5 ml of saline to a slant culture of Escherichia coli. Gently scrape the surface and suspend bacteria uniformly. Add 2 or 3 drops of this suspension to the middle of the warmed agar plate. Spread the bacteria on the surface of the agar with a loop. Depending on the specimen, incubation should be as follows: (CSF or other nervous system material- 37C; other tissues at 30C). After the fluid/specimen has been absorbed, seal the plates with a 5 to 6in strip of Parafilm; incubate the plate inverted (room air).
Using the low power objective (10X), examine the plates for amebae (cysts or trophozoites) every day for 10 days. Thin, linear tracks (areas where amebae have ingested the bacteria) might also be seen. Complete directions can be found in Diagnostic Medical Parasitology, 5th ed.
Therapy: Current therapy for Acanthamoeba meningoencephalitis includes amphotericin B and sulfadiazine or sulfisoxazole or pentamidine isethionate. Treatment is somewhat problematic and amphotericin B may be ineffective. Skin ulcers have been treated with systemic administration of combination therapy pentamidine isethionate IV for one month and oral itraconazole for eight months. The skin ulcers can also be cleaned twice daily with chlorhexidine gluconate solution and treated with topical application of 2% ketoconazole cream.
References:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.