

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
Presentation of Diagnostic Quiz #76
***Reminder: Slides are copyrighted and cannot be copied for publication.
A 46 year old female, originally from Los Angeles, was seen in the clinic with a three week history of diarrhea and general malaise. This patient had an extensive travel history, visiting numerous countries on a regular basis. These trips included Europe, Latin America, Asia, Africa, and throughout North America. She often took side trips stayed in both expensive and relatively inexpensive accommodations. She also liked to eat many of the local dishes on her travels. Apparently, she had no underlying health problems. On presentation to the clinic, she was complaining of intermittent diarrhea, a weight loss of approximately 10 pounds, and general malaise.
Routine stool examinations for parasites (three ova and parasite examinations) revealed the following:
Structures (x1,000)
QUESTIONS:
Scroll Down for Answer and Discussion
ANSWER AND DISCUSSION OF DIAGNOSTIC QUIZ #76
The images presented in Diagnostic Quiz #76 are the following:
ANSWERS TO QUESTIONS:
COMMENTS ON THE PATIENT:
This case represents a situation in which the cause of the patient's symptoms may be something other than an infection with intestinal parasites. Another possibility is that the routine Ova and Parasite Examination (O&P) did not allow detection and identification of the particular parasite involved.
COMMENTS ON THE METHOD LIMITATIONS:
It is always recommended that a thorough examination be performed (minimum of two specimens for O&P examinations - three is even better) before reporting the patient as "No Parasites Seen." Also, remember that the routine O&P examination does not allow the detection of organisms like Cryptosporidium parvum, Cyclospora cayetanensis, or the microsporidia. A statement listing the method limitations should be included in the report to the physician. In spite of these method limitations with some of the coccidia, the coccidian, Cystoisospora belli, can usually be identified in the concentration sediment wet smear examination. For confirmation of the actual pathogen, Entamoeba histolytica vs nonpathogenic E. dispar, molecular methods can be used; without the presence of ingested RBCs in the trophozoite cytoplasm, differentiation is not possible microscopically as E. histolytica. A report comment can be added indicating the inability to differentiate the true pathogen microscopically without the presence of ingested RBCs.
COMMENTS ON THE IMAGES:
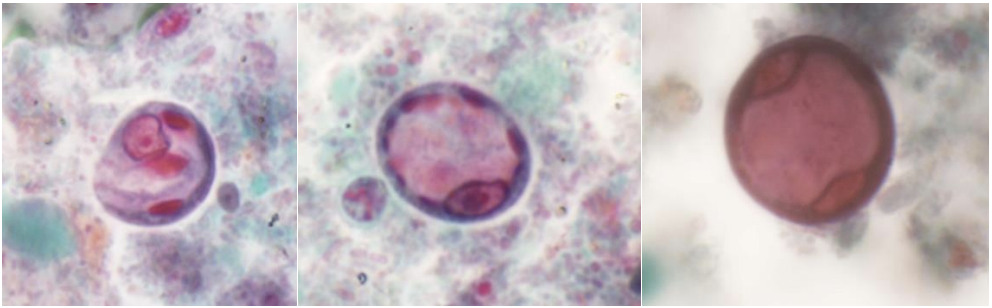
E. coli cysts do not tend to stain well on the permanent stained smear (fixative does not penetrate the cyst wall very well, even using mercury-based fixatives), but their color tends to be more blue or purple (normal cyst); if the cyst is very shrunk, it may even appear pink to red to purple in color (Wheatley's trichrome stain), as seen below.
Wheatley's trichrome stain (permanent stained smear) (x1,000)
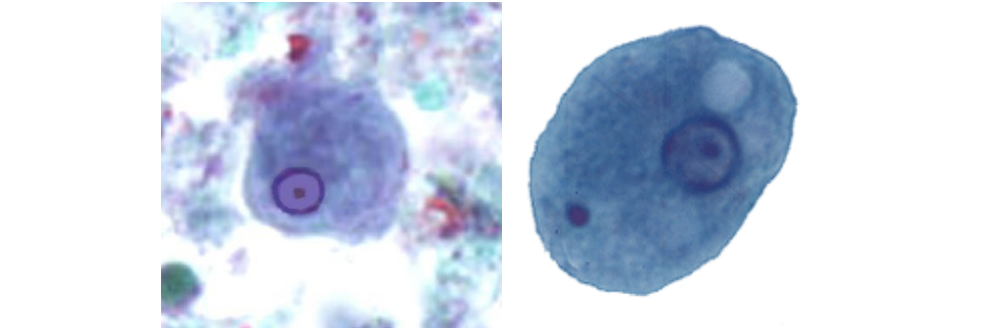
Here are some examples of Entamoeba histolytica/E. dispar trophozoites and cysts, as well as some examples of E. coli cysts.
The image on the left is an E. histolytica/E. dispar trophozoite (note the ratio of the nucleus to cytoplasm is about 1:9 and the next two images are E. histolytica/E. dispar cysts (note the nuclei are about the same size).
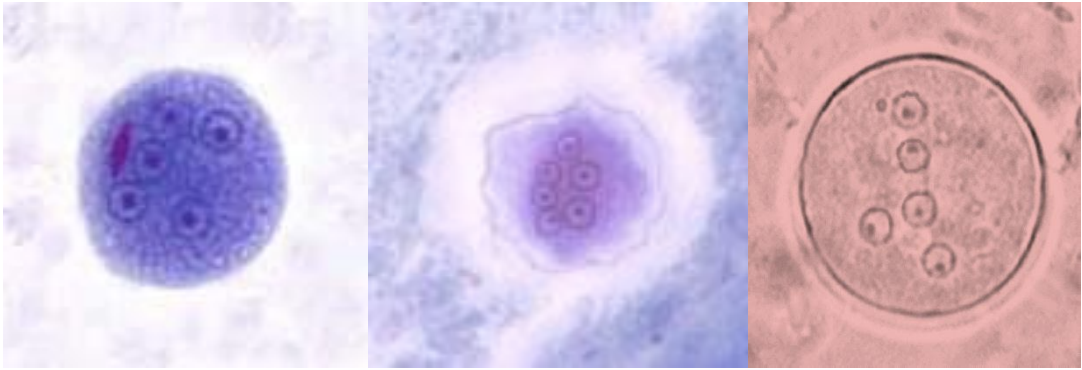
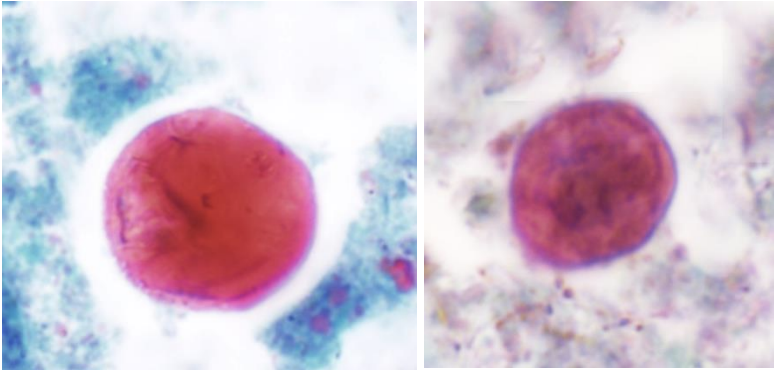
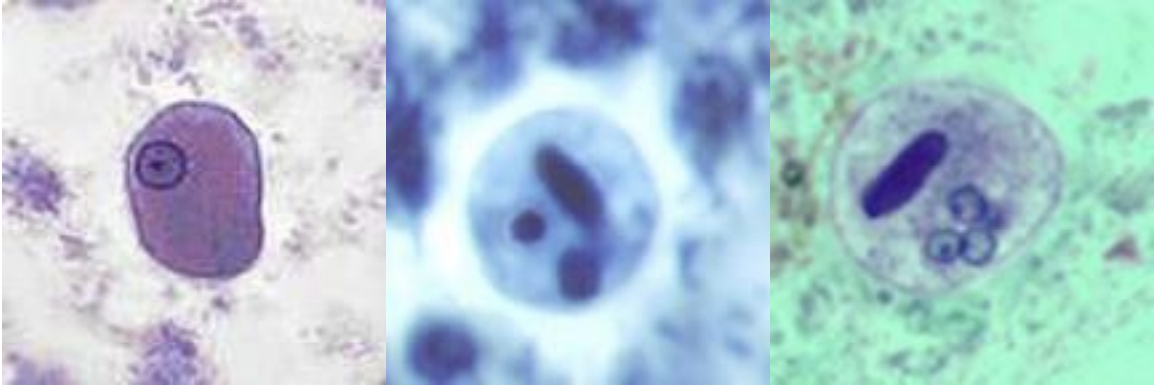
The image on the left is an E. coli cyst (Wheatley's trichrome stain - permanent stained smear); note the nuclei are about the same size. The image in the middle is also an E. coli cyst (shrunk, Wheatley's trichrome stain). The image on the right is an E. coli cyst on an iodine wet mount; again, note the consistency of the nuclear size. Depending on the amount of iodine added to the wet mount, the cyst can appear to be yellow to gold to orange to almost reddish brown.
References:
Garcia, L.S. 2016. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.
Leber, A.L. and S.M. Novak. 2003. Intestinal and Urogenital Amebae, Flagellates, and Ciliates In: Murray, P.R., E.J. Baron, J.H. Jorgensen, M.A. Pfaller, and R.H. Yolken (eds). Manual of Clinical Microbiology, 8th ed, vol 2, ASM Press, Washington, D.C.
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.