Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
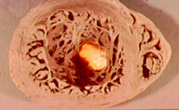
A 43-year-old immigrant male from Brazil was admitted to the hospital with a long history of cardiac arrhythmias. Unfortunately, he died suddenly, very soon after admission. Autopsy findings revealed an apical ventricular aneurysm, severe cardiac inflammatory responses in numerous areas and representative organisms as seen below.
Please comment on the possible diagnosis related to the history, the patient's clinical symptoms and the autopsy findings.
1. Heart, gross section (note light under apex of heart, indicating ventricular aneurysm); also note the thickened wall of the heart |
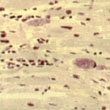
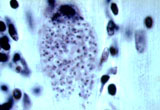
2. "Nests" of organisms |
Figure 1. From a Pictorial Presentation of Parasites: A cooperative collection prepared and/or edited by H. Zaiman.
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #13
The images presented in Diagnostic Quiz #13 are the following:
Comment: This is a case of a man who was infected with Trypanosoma cruzi.
American trypanosomiasis (Chagas' disease) is a zoonosis caused by T. cruzi discovered in Brazil in 1909 by Carlos Chagas, who described the entire life cycle in reservoir hosts. T. cruzi causes an acute or chronic parasitemia and invades the cells of many organs (e.g., heart, esophagus, and colon). Chagas' disease is one of the major health problems in Latin American countries. It is estimated that there are 100 million persons at risk of infection, of whom 16 million to 18 million are actually infected. There are approximately 50,000 deaths per year due to Chagas' disease. In certain endemic areas, approximately 10% of all adult deaths are due to Chagas' disease.
The infective organism is transmitted to humans through the bug’ fecal material scratched into the bite wound caused by the reduviid bugs (triatomids, kissing bugs, or conenose bugs). Humans are infected when metacyclic trypomastigotes are released with the feces while the insect is taking a blood meal, and the feces are rubbed or scratched into the bite wound or onto mucosal surfaces, an action stimulated by the allergic reaction to the insect's saliva. Upon entry into the wound, the metacyclic forms invade local tissues, transform to the amastigote stage, and begin to multiply within the cells. In humans, T. cruzi can be found in two forms, amastigotes and trypomastigotes. The trypomastigote does not divide in the blood but carries the infection to all parts of the body. The amastigote form multiplies within virtually any cell, preferring cells of the reticuloendothelial system, cardiac muscle, skeletal muscle, smooth muscle, and neuroglia.
The trypomastigote is spindle shaped, approximately 20 mm long, and characteristically assumes a ``C'' or ``U'' shape in stained blood films. Trypomastigotes occur in the blood in two forms, a long slender form and a short stubby one. The nucleus is situated in the center of the body, with a large oval kinetoplast located at the posterior extremity. The kinetoplast consists of a small blepharoplast and a large oval parabasal body. A flagellum arises from the blepharoplast and extends along the outer edge of an undulating membrane until it reaches the anterior end of the body, where it projects as a free flagellum. When the trypomastigotes are stained with any of the blood stains, the cytoplasm stains blue and the nucleus, kinetoplast, and flagellum stain red or violet.
In addition to contracting T. cruzi infections through the insect's bite wound or exposed mucous membranes, one can be infected by blood transfusion, organ transplantation, placental transfer and accidental ingestion of parasitized reduviid bugs. The clinical syndromes associated with Chagas' disease can be broken down into acute and chronic phases. The acute phase is the result of the first encounter of the patient with the parasite whereas the chronic phase is the result of late sequelae. In children under the age of 5, the disease is seen in its severest form, whereas in older children and adults, the disease is milder and is commonly diagnosed in the subacute or chronic form rather than in the acute form.
Acute-phase symptoms are usually seen in younger children and are less obvious in older individuals because of the nonspecific nature of the symptoms and the lack of availability to health care. Acute systemic signs occur around week 2 to 3 of infection and are characterized by the following: high fevers, which may be intermittent, remitting, or continuous; hepatosplenomegaly; myalgia; erythematous rash; acute myocarditis; lymphadenopathy; and subcutaneous edema of face, legs, and feet. There may be signs of CNS involvement including meningoencephalitis which has a very poor prognosis. Myocarditis is manifested by electrocardiographic changes, tachycardia, chest pain, and weakness. Amastigotes proliferate within the cardiac muscle cells and destroy the cells, which causes conduction defects and a loss of heart contractility. Death may occur due to myocardial insufficiency or cardiac arrest.
Symptoms of the chronic phase are related to the damage sustained during the acute phase of the disease. Chronic Chagas' disease may develop years or decades after undetected infection or after the diagnosis of acute disease. The most frequent clinical sign of chronic Chagas' disease is cardiomyopathy manifested by cardiomegaly and conduction changes. Because there are so few organisms isolated or seen in heart tissue, much of the cardiac tissue destruction is thought to be related to autoimmune antibodies possible due to crossreactivity to related T. cruzi antigens. The clinical course may vary from heart failure to a slow but continuing loss of cardiac function, with possible ventricular rupture and thromboemboli. Although it is less common than cardiac involvement, patients from certain areas are more likely to have dilation of the digestive tract with or without cardiomyopathy. These symptoms are most frequently seen in the esophagus and colon as a result of neuronal destruction. Megaesophagus characterized by dysphagia, chest pain, regurgitation and malnutrition is related to loss of contractility of the lower esophagus. Hypersalivation may occur leading to aspiration with repeated bouts of aspiration pneumonia. Megacolon results in constipation, abdominal pain and the inability to discharge feces. In some individuals, there may be acute obstruction leading to perforation, septicemia and death.
Trypomastigotes may be detected in blood by using thin and thick blood films or by buffy coat concentration techniques. T. cruzitrypomastigotes are usually ``C'' or ``U'' shaped on fixed blood films and have a large oval kinetoplast at the posterior end. Histologic examination of biopsies may also be done. Aspirates, blood, and tissues can also be cultured, which is valuable in detecting low-grade parasitemias. In endemic areas where reduviid bugs are readily available, xenodiagnosis can be used to detect light infections; this technique is most valuable for chronic infections when there are few trypomastigotes in the blood. Trypanosome-free bugs are allowed to feed on individuals suspected of having Chagas' disease. If organisms are present in the blood meal, the parasites will multiply and be detected in the bug's intestinal contents, which should be examined monthly for flagellated forms over a period of 3 months.
In the chronic phase of Chagas' disease, trypomastigotes are very rare or absent in the peripheral blood except during febrile exacerbations. Diagnosis depends primarily on culture xenodiagnosis or serologic tests. Some individuals with chronic Chagas' disease may have a depressed humoral immune response, being serologically negative. This response has been correlated with specific zymodemes. Chronic disease should be considered in individuals from endemic areas who show signs of cardiomegaly, cardiac conduction defects, severe constipation, or dysphagia.
T. cruzi: amastigotes in tissue |
T. cruzi: trypomastigote, thin blood film |
T. cruzi: culture stages |
T. cruzi: xenodiagnosis |
T. cruzi: triatomid bug, vector |
References:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.