Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 47 year old male was admitted to the hospital with complaints of severe mid-epigastric pain that had become worse over a period of about a week. This patient had received prednisone over the course of several years and the dose had been increased two months before. Previous diagnostic testing included an O&P examination, which was reported as "No Parasites Seen."
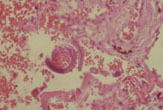
He was treated with supportive care for epigastric pain and developing pneumonia, but failed to improve. He became comatose and died three days later. Autopsy findings included the following image (colon):
What infection most likely matches this image? Based on the history why might there be no evidence of eosinophilia?
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #27
The images presented in Diagnostic Quiz #27 are the following:
|
|
Strongyloides stercoralis (rhabditiform larvae): found in stool specimens. Note the short buccal capsule (mouth opening seen in left image) and large packet of genital primordium cells (seen in both images).
|
|
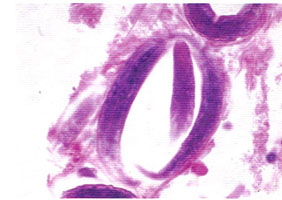
Strongyloides stercoralis (larva in lung - left image); slit in the tail of filariform (infective) larva (right image).
Comments on the Patient: This case represents a generalized infection with Strongyloides stercoralis involving lungs, liver, peritoneum, small intestine, colon, respiratory diaphragm, heart, lymph nodes, skeletal muscle and periadrenal and peripancreatic fat. There was generalized peritonitis. Intact rhabditiform and filariform larvae of S. stercoralis were seen in the tissues and in stool. It is unfortunate that additional O&P examinations were not performed during this hospital admission.
Comments on Strongyloides stercoralis: Strongyloidiasis most often reported in warm climates, but has been found in temperate and cold climates. It overlaps the same geographic range as hookworm infections. The disease is contracted by penetration of the filariform larvae into the skin by contact with infected soil, by autoinfection or by fecal-oral contamination. Generalized disease may present in many ways: paralytic ileus, an acute surgical abdomen, asthma, and as a protein-losing enteropathy with malabsorption. It should be considered in patients with bronchopneumonia and accompanying abdominal symptoms.
Findings of bilateral pulmonary disease were due to extensive intraalveolar hemorrhage and interstitial pneumonia; numerous larval forms were present in the lung. When young worms break out of the pulmonary capillary into the alveoli, hemorrhage and cellular infiltration into the air sacs and bronchioles result.
High eosinophilia may or may not be present. In this case, no eosinophils were noted (eosinopenia can occur in the hyperinfection syndrome = poor prognostic sign).
Malnutrition, lymphoma, treatment with immunosuppressives, and corticosteroid therapy are predisposing factors in strongyloidiasis. It is also very important to consider this infection in military personnel and travelers who may have been in an endemic area many years before. More than 30 to 40 years after acquisition of the original infection, persistent, undiagnosed disease can be found in these individuals. If, for any reason, they become immunocompromised, the result can be disseminated disease leading to the hyperinfection syndrome and death.
In situations in which autoinfection occurs, some of the rhabditiform larvae that are within the intestine develop into the filariform larvae while passing through the bowel. These larvae can then reinfect the host by 1) invading the intestinal mucosa, traveling via the portal system to the lungs, and returning to the intestine, or 2) being passed out in the feces and penetrating the host on reaching the perianal or perineal skin.
Clinical Disease: Pathology present in strongyloidiasis can vary, both in severity and areas of the body involved. Some individuals may remain totally asymptomatic, with the only abnormal clinical finding being a peripheral eosinophilia.
Cutaneous: Initial skin penetration usually causes very little reaction, although there may be some pruritus and erythema if the number of penetrating larvae is high. With repeated infections, the patient may mount an allergic response that will prevent the parasite from completing the life cycle. The larvae may be limited to skin migration or larva migrans. The term larva currens ("racing larvae") was proposed in 1958 and is now generally accepted for cases of strongyloidiasis in which there is one or more rapidly progressing linear urticarial tracks starting near the anus. There is speculation that some of these cases may involve larvae of other species of Strongyloides. These tracks may progress as fast as 10 cm/hour, with an intermittent movement, usually on the thighs. Onset is sudden and the lesions may disappear within 12 to 18 hours.
Pulmonary: Larval migration through the lungs may stimulate symptoms, depending on how many larvae are present and the intensity of the host's immune response. Some patients may be asymptomatic, while others may present with pneumonia. With a heavy infective dose or in the hyperinfection syndrome, individuals often develop cough, shortness of breath, wheezing, fever, and transient pulmonary infiltrates (Loeffler's syndrome). There have also been cases reported where the larvae can be found in the sputum.
Intestinal: In heavy infections, the intestinal mucosa may be severely damaged with sloughing of tissue, although this type of damage is unusual. Symptoms may mimic peptic ulcer with abdominal pain, which may be localized in the right upper quadrant. Radiographic findings may mimic Crohn's disease of the proximal small intestine. In an immunocompetent patient, there is a leukocytosis with a peripheral eosinophilia of 50-75%, while in chronic cases the eosinophilia may be much lower. Some of these chronic infections have lasted over 30 years as a result of the autoinfective capability of the larvae. One case of chronic strongyloidiasis persisted for approximately 65 years.
Hyperinfection Syndrome: Autoinfection is probably the mechanism responsible for long-term infections that persist years after the person has left the endemic area. The parasite and host reach a status quo so that neither suffers any serious damage. If for any reason this equilibrium is disturbed and the individual becomes immunosuppressed, then the infection proliferates, with large numbers of larvae being produced and found in every tissue of the body. Several conditions predispose an individual to the hyperinfection syndrome and include the increased use of immunosuppressive therapy. In addition to the actual tissue damage from the migrating larvae, the patient may die from sepsis, primarily as a result of intestinal flora. Other causes of death may include peritonitis, brain damage, or respiratory failure.
Reactive arthritis: Few cases of reactive arthritis have been reported and the number of cases may be underestimated. A case of reactive arthritis combined with uveitis associated with a long-standing, heavy Strongyloides infection is reported in a 32-year-old HTLV-1 positive patient. Treatment with thiabendazole and ivermectin resulted in rapid improvement.
NOTE: Debilitated or compromised patients should always be suspected of having strongyloidiasis, particularly if there are unexplained bouts of diarrhea and abdominal pain, repeated episodes of sepsis and/or meningitis with intestinal bacteria or unexplained eosinophilia. However, a recent comparative study on the occurrence of Strongyloides in 554 AIDS and 142 non-AIDS patients demonstrated a similar prevalence of infection in both groups, thus indicating no significant statistical differences.
Key Points - Laboratory Diagnosis:
Treatment: Thiabendazole has been used in the past; in some cases, repeated or extended (one week) therapy may be necessary, and the cure rates range from 55 to 100%. Patients with the hyperinfection syndrome should be hospitalized during therapy for proper monitoring. Ivermectin has become more widely used in the last few years.
Epidemiology and Prevention: Contact with contaminated infective soil, feces, or surface water should be avoided. Individuals found to have the infection should be treated. All patients who are going to receive immunosuppressive drugs should be screened for strongyloidiasis before therapy.
Final Comments: Strongyloidiasis is endemic at least as far north as New York City. It is very likely that endemic foci also exist in other metropolitan areas within the United States and cases similar to the one presented here could occur any place within the country. This was a case of disseminated strongyloidiasis presenting as acute abdominal distress in an adult who had been receiving immunosuppressive therapy.
References:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.