

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
***Reminder: Slides are copyrighted and cannot be copied for publication.
A patient is a 39 year-old male who presented to the clinic with complaints of right upper quadrant pain. He had no medical problems or complaints in the past. Although he had spent many years in Spain living with family, he had been living in the United States for the last several years. About a year prior to the clinic visit, he began experiencing dull right upper quadrant abdominal pain, usually a couple of hours after eating. He had no fever, chills, rashes, weight loss, nausea or vomiting or food intolerance. In the Basque region of Spain, when visiting his grandfather he lived on the second floor of the house, the first floor being a patio/shed that was often full of domestic animals such as pigs, sheep, goats, and dogs. Although his laboratory findings were all normal, a liver scan showed a 7 cm defect.
Based on the patient's history, what do you think the most likely diagnosis might be? How do you think the patient acquired the infection? If surgery is performed, what are some of the key issues to consider? Prevention of the disease would include what measures?
At surgery, the following objects were removed from the cyst. Does this image assist you in making the diagnosis? Why or why not?
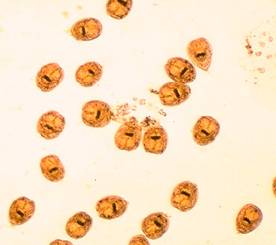

The structures in the left image were photographed using the 40x high dry objective; the structures in the right image were photographed using the 100x oil immersion objective.
(Scroll Down for Answers and Discussion)
ANSWER AND DISCUSSION OF DIAGNOSTIC QUIZ #56
ANSWERS TO QUESTIONS:
The left image is of hydatid sand (immature scolices), and the right image is of individual hooklets. Note the dark area on each scolex; this are represents the hooklets that are on each immature scolex.
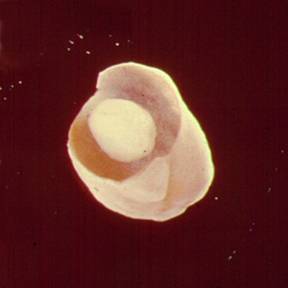
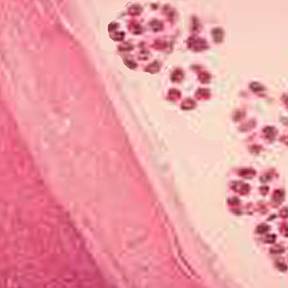
Below you will see an image of a daughter cyst that was removed at surgery (left image), as well as the various cyst layers seen in a routine histology section (note the daughter scolices - multiple purple small round bodies) (right image).
The clinical and radiologic pictures are almost pathognomonic of hydatid disease with Echinococcus granulosus. The patient most likely acquired the infection by the accidental ingestion of infective eggs from tapeworms within the dog's intestine. When the proglottids are passed in stool, the eggs are then on the ground, etc. The risk of infection depends to a high degree on the association between humans and dogs. Those at high risk include populations where dogs are used to herd sheep and are also intimate members of the family, often having unrestricted access to the house and family members.
If surgery is used to remove the cyst, it is imperative that care be taken to prevent spillage of the cyst contents. If this occurs, then the viable scolices and/or parts of the germinal layer can be disseminated and regrow in other parts of the body. Also, prior to cyst removal at surgery, various solutions can be instilled into the cyst cavity in order to kill the larvae and/or germinal tissue layer.
COMMENTS ON THE PATIENT:
This patient most likely acquired the infection years before, and based on the cyst growth, finally began to have symptoms. The majority of hydatid cysts occur in the liver, causing symptoms that may include chronic abdominal discomfort, occasionally with a palpable or visible abdominal mass. Liver cysts tend to occur more frequently in the right lobe.
COMMENTS ON DIAGNOSTIC METHODS:
Hydatid cysts should be considered in patients with abdominal masses with no clearly defined diagnosis. Although eosinophilia is present in 20 to 25% of patients, it is merely suggestive. Many asymptomatic cysts are first discovered after radiologic studies. The cyst will usually have a well-defined margin with occasional fluid level markings.
Once the cyst is discovered and surgical removal is selected as the approach, some of the cyst fluid can be aspirated and submitted for microscopic examination to detect the presence of hydatid sand, thus confirming the diagnosis. This procedure is definitely not without risk because of possible fluid and/or tissue leakage or dissemination. Cyst aspiration is usually performed at the time of surgery.
A drop of centrifuged fluid can be placed on a slide; another slide can be placed on top of the drop. The two slides can be rubbed back and forth over the fluid. The grating of the hooks on the glass may be felt and heard (hydatid sand sounds like glass grating on sand grains). Of course, if the individual scolices are intact, routine microscopic examination of the centrifuged fluid as a wet mount will confirm the diagnosis. If the cyst is sterile (no daughter cysts or scolices), the diagnosis could be confirmed histologically from the cyst wall.
A number of options are available for treatment of cystic echinococcosis, including surgery, puncture aspiration injection reaspiration (PAIR), and chemotherapy. Surgery is generally considered the treatment of choice for a complete cure, although this approach is limited to unilocular cysts in operable body sites. In cases where multiple cysts are present in several different sites or in patients with a high surgical risk, PAIR and/or chemotherapy are considered appropriate options.
Because there is always the risk of cyst fluid spillage during surgery, pre- and/or post-operative use of chemotherapy may be appropriate. Chemotherapy with albendazole or mebendazole offers the advantage of reducing the risk of disease recurrence and intraperitoneal seeding of infection that may develop via cyst rupture and spillage occurring spontaneously or during surgery or needle drainage. Surgery is normally reserved for patients with hydatid cysts refractory to PAIR due to advanced hydatid disease or secondary bacterial infection or for patients with cyst-biliary communication or obstruction.
REFERENCES
Eckert, J., and P. Deplazes. 2004. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin. Microbiol. Rev. 17:107-135.
Garcia, LS, 2016. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, DC.
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.