Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 45-year-old naval engineer presented to his physician with swelling of his face and legs. He reported having diarrhea and general indigestion about two weeks before. He also indicated he had a bad upper respiratory infection about a month before. On the day he presented to the physician, during the discussion he commented that occasionally he saw undigested food in his stool. The patient works for an engineering firm that has multiple contracts throughout the Philippines, Taiwan, and Australia. During the previous six months, he had visited all of these areas, usually eating most of the local food specialties, including raw fish and raw vegetables served in salads. He had no underlying health problems.
On presentation, the patient appeared in no particular distress; however, there was some facial edema and pitting edema of the legs. The lungs and heart were normal.
His laboratory findings included a marked eosinophilia and leukocytosis. With his history of diarrhea, relevant travel, and eating habits, examinations for parasites revealed the following from the O&P examination:
|
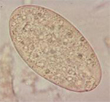
This object measured about 140 by 70 microns and was easily seen in the saline wet preparation examination.
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #49
The image presented in Diagnostic Quiz #49 is the following:
Comment:
The patient's symptoms will reflect the phase of the infection, as well as the number of parasites present in the host. In light infections, the adult worms inhabit the duodenum and jejunum; in heavy infections they may be found in the stomach and most of the intestinal tract. The attachment of worms to the mucosal wall produces local inflammation with hypersecretion of mucus, hemorrhage, ulceration, and possible abscess formation. In heavy infections, the worms may cause bowel obstruction, acute ileus, and absorption of toxic or allergic worm metabolites, producing general edema and ascites. Facial edema may occur as a result of hypoalbuminemia secondary to malabsorption or protein-losing enteropathy. A marked eosinophilia and leukocytosis are commonly seen.
Few symptoms are seen in light infections, but in heavier infections, the patient may have abdominal pain and diarrhea. In heavy infections, the stools are profuse and yellow-green, and contain increased amounts of undigested food. The symptoms may be confused with those of giardiasis, peptic ulcer, or other causes of bowel obstruction. Depending on the worm burden, the infection can be associated with severe wasting, prostration, and can lead to death.
Life Cycle:
Adult worms, which live in the small intestine of pigs and humans, produce unembryonated eggs that are passed into the environment with the feces. The eggs are operculated, large, ovoid, and yellow-brown. Depending on the temperature, the eggs embryonate within about 3 to 7 weeks. Once in the water, the mature miracidium hatches from the egg to infect the snail intermediate host; then it begins to develop into a first-generation sporocyst. Two generations of rediae are produced, and eventually cercariae are liberated from the snail. Cercariae encyst on water vegetation, such as water caltrops, water chestnuts, and water bamboo where they develop into metacercariae in about 4 weeks. Humans are infected by ingestion of uncooked aquatic vegetation on which metacercariae are encysted. Metacercariae excyst in the duodenum, attach to the duodenal or jejunal mucosa, and develop into adult worms within about 3 months.
Epidemiology and Control:
Reservoir hosts include dogs, pigs, and rabbits. The infection is commonly found in Bangladesh, Cambodia, central and southern China, India, Indonesia, Laos, Malaysia, Pakistan, Taiwan, Thailand, and Vietnam; infections have also been reported in Japan. Drainage of farm waste, use of manure for cultivation, and defecation in or near ponds or lakes that contain appropriate snails, with water plants acting as vectors, allows the life cycle to continue. To prevent the infection, plants should be cooked or immersed in boiling water for a few seconds before they are eaten or peeled. The use of unsterilized night soil for fertilizer should be prohibited.
Fasciolopsis buski Key Points - Laboratory Diagnosis
Treatment: Praziquantel is the drug of choice and can be given in a single dose of 40 mg/kg at bedtime. Another option would be albendazole at 400 mg twice a day for 3 days.
|
|
|
Three images of Fasciolopsis buski eggs from a routine stool examination (wet preparation). The first image is the egg seen above in a saline wet preparation (note the presence of the operculum at the top of the egg - hard to see). The middle image shows an egg photographed in a saline wet mount, but at a somewhat higher magnification (note the operculum at the upper end). The image on the far right shows an egg photographed from an iodine wet mount; the operculum is visible at the top of the egg.
References:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.