Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 6 year old girl was admitted to the hospital in a coma. The patient was normally a healthy child with no prior significant medical history. Several days prior to admission the family had been vacationing at a lake in the southern United States. Everyone had been swimming and boating during the previous week. Several days before admission, she had complained of some vague upper respiratory distress and a sore throat. On the day prior to admission, her mother indicated she had complained of a stiff neck and headache; she also had a fever. On the day of admission, she became very confused and lapsed into a coma.
On physical examination, her neck was stiff and her pupils reacted sluggishly; her temperature was 104°F.
The CSF was hemorrhagic and contained many neutrophils. Although there was some debris on the smear, the Gram stain was read as negative.
QUESTION 1: What laboratory procedure should be performed immediately and why?
QUESTION 2: If the procedure was positive, what would you expect to see?
QUESTION 3: Treatment should be started immediately with what and why?
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #25
QUESTION 1: The CSF should be examined as a wet mount (not in a counting chamber), looking for motile amebic trophozoites. The specimen can be centrifuged or unspun; do not refrigerate. Amebic trophozoites can mimic neutrophils in a counting chamber, but characteristic motility can be seen on a slide with a coverslip.
QUESTION 2: In a positive wet mount, motile trophozoites of free-living amebae (probably Naegleria fowleri) would be seen. The pseudopodia will be rounded (non-spiky) and motility will be visible unless the organisms are cold or dead.
QUESTION 3: The only drug that appears to be effective is amphotericin B. Very few patients have survived this infection; two patients responded to amphotericin B. Rare cases have also received miconazole and, in one case, rifampin.
Comment: Infections of the central nervous system (CNS) caused by free-living amebae have been recognized only since the mid-1960s, and our understanding of this disease process is still incomplete. One type of meningoencephalitis (PAM) is a fulminant and rapidly fatal disease that mainly affects children and young adults. The disease closely resembles bacterial meningitis but is caused by Naegleria fowleri, an organism found in moist soil and freshwater habitats.
Life Cycle: There are trophozoite and cyst stages in the life cycle, the stage primarily depending on environmental conditions. Trophozoites can be found in water or moist soil and can be maintained in tissue culture or other artificial media.
The trophozoites can occur in two forms, ameboid and flagellate. Motility can be observed in hanging drop preparations from cultures of cerebrospinal fluid (CSF); the ameboid form (the only form recognized in humans) is elongate with a broad anterior end and tapered posterior end. The size ranges from 7 to 20 μm. The diameter of the rounded forms is usually 15 μm. There is a large, central karyosome and no peripheral nuclear chromatin. The cytoplasm is somewhat granular and contains vacuoles. The ameboid-form organisms change to the flagellate form when they are transferred from culture or teased from tissue into water and maintained at a temperature of 27 to 37°C. The change may occur very quickly (within hours), or it may take as long as 20 h. The flagellate form is pear shaped, with two flagella at the broad end. Motility is typical, with either spinning or jerky movements. These flagellate forms do not divide, but when the flagella are lost, the ameboid forms resume reproduction. Cysts from nature and from agar cultures look the same and have a single nucleus almost identical to that seen in the trophozoite. The shape is generally round, measuring from 7 to 10 μm, and there is a thick double wall.
Clinical Disease: Primary amebic meningoencephalitis (PAM) caused by N. fowleri is an acute, suppurative infection of the brain and meninges. In humans, with extremely rare exceptions, the disease is rapidly fatal. The period between contact with the organism and onset of clinical symptoms such as fever, headache, and rhinitis may vary from 2 to 3 days to as long as 7 to 15 days. The amebae may enter the nasal cavity by inhalation or aspiration of water, dust, or aerosols containing the trophozoites or cysts. The organisms then penetrate the nasal mucosa, probably through phagocytosis of the olfactory epithelium cells, and migrate via the olfactory nerves to the brain. Early symptoms include vague upper respiratory distress, headache, lethargy, and occasionally olfactory problems. The acute phase includes sore throat, stuffy blocked or discharging nose, and severe headache. Progressive symptoms include pyrexia, vomiting, and stiffness of the neck. Mental confusion and coma usually occur approximately 3 to 5 days prior to death. The cause of death is usually cardiorespiratory arrest and pulmonary edema. PAM can resemble acute purulent bacterial meningitis and may be difficult to differentiate, particularly in the early stages. Unfortunately, if the CSF Gram stain is interpreted incorrectly (identification of bacteria as a false positive), the antibacterial therapy has no impact on the amebae and the patient will usually die within several days. Extensive tissue damage occurs along the path of amebic invasion; the nasopharyngeal mucosa shows ulceration, and the olfactory nerves are inflamed and necrotic. Hemorrhagic necrosis is concentrated in the region of the olfactory bulbs and the base of the brain. Organisms can be found in the meninges, perivascular spaces, and sanguinopurulent exudates.
Diagnosis: Clinical and laboratory data usually cannot be used to differentiate pyogenic meningitis from PAM, so the diagnosis may have to be reached by a process of elimination. A high index of suspicion is often mandatory for early diagnosis. Although most cases are associated with exposure to contaminated water through swimming or bathing, this is not always the case. The rapidly fatal course of 4 to 6 days after the beginning of symptoms (with an incubation period of 1 day to 2 weeks) requires early diagnosis and immediate chemotherapy if the patient is to survive. Analysis of the CSF will show decreased glucose and increased protein concentrations. Leukocytes may range from several hundred to >20,000 cells per mm3. Gram stains and bacterial cultures of CSF will be negative.
A definite diagnosis could be made by demonstration of the amebae in the CSF or in biopsy specimens. Either CSF or sedimented CSF should be placed on a slide, under a coverslip, and observed for motile trophozoites; smears can also be stained with a blood stain. CSF, exudate, or tissue fragments can be examined by light microscopy or phase-contrast microscopy. Care must be taken not to mistake leukocytes for actual organisms or vice versa. It is very easy to confuse leukocytes and amebae, particularly when one is examining CSF by using a counting chamber, hence the recommendation to use just a regular slide and coverslip. Motility may vary, so the main differential characteristic is the spherical nucleus with a large karyosome.
Specimens should never be refrigerated prior to examination. When centrifuging the CSF, spin at low speeds (250 x g) so that the trophozoites are not damaged. Although bright-field microscopy with reduced light is acceptable, phase microscopy, if available, is recommended. Use of smears stained with a blood stain or a Giemsa-Wright's stain combination can also be helpful. If N. fowleri is the causative agent, trophozoites only are normally seen. If the infecting organism is Acanthamoeba spp., then cysts may also be seen in specimens from CNS disease. Unfortunately, most cases are diagnosed at autopsy; confirmation of these tissue findings must include culture and/or special staining using monoclonal reagents in indirect fluorescent antibody procedures. Organisms can also be cultured on nonnutrient agar plated with Escherichia coli.
Key Points - Laboratory Diagnosis:
Epidemiology and Control: Over 175 presumptive or proven cases of PAM have been reported in the literature, including cases from the United States (86 cases as of January, 1998), Ireland, England, Belgium, Czechoslovakia, Australia, New Zealand, Brazil, and Zambia. Clinical patient histories indicate exposure to the organism via freshwater lakes or swimming pools shortly before onset; patients had been previously healthy with no specific underlying problems. Pathogenic Naegleria organisms have also been isolated from nasal passages of individuals with no history of water exposure, thus suggesting the possibility of airborne exposure.
The first isolations of the environmental strains of pathogenic N. fowleri were reported from water and soil in Australia and from sewage sludge samples in India. Detection of N. fowleri in heated discharge water has been reported in Belgium and Poland. Since then, there have been additional reports describing isolations of virulent or avirulent strains of N. fowleri from the environment. Studies in Belgium have clearly indicated that N. fowleri strains are present in artificially heated waters (power plant warm discharge), and studies in the United States have indicated that virulent strains are also found in lakes in geographic latitudes with water temperatures of 14 to 35°C that are totally isolated from any source of thermal discharge. These data suggest that the presence of pathogenic or potentially pathogenic amebic strains may depend on both climate and modification of the natural environment. The ability of the cysts to survive under various environmental conditions has been investigated by several workers. These findings suggest that N. fowleri cysts produced in the warm summer months may survive the winter and are capable of growth in the following summer.
General preventive measures include public awareness of potential hazards of contaminated water. It has been recommended that warm discharge water not be used for sports and recreational purposes, particularly since DNA restriction fragment profiles of environmental strains and human isolates were homogeneous.
Treatment: Only 3 patients of more than 175 with presumptive or parasitologically proven cases of PAM had survived this infection outside of the United States by the 1970s. Seidel et al. reported on one case within California in which the patient was successfully treated with amphotericin B, miconazole, and rifampin. There was a synergistic effect with miconazole and amphotericin B in vitro; however, rifampin was ineffective. The patient received intrathecal and intravenous injections of the drug. Dexamethasone and phenytoin were also given to this patient to decrease intracranial pressure and seizure, respectively. Naegleria infections have also been treated successfully with amphotericin B, rifampin, and chloramphenicol; amphotericin B, oral rifampin and oral ketoconazole; and amphotericin B alone.
|
|
|
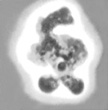
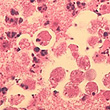
These images are representative of Naegleria fowleri. The image on the left is a trophozoite as seen in a wet mount of CSF or culture (high magnification). The middle image is a low power image of brain tissue (routine histology). The image on the right is a higher magnification of an organism in brain tissue. In these images, note the large karyosome with no peripheral nuclear chromatin.
|
|
|
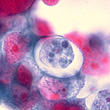
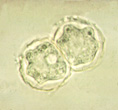
These images are representative of Acanthamoeba spp. The image on the left contains trophozoites as seen in a wet mount of CSF (granulomatous amebic meningoencephalitis - GAE) or from culture (high magnification). Note the sharp, spiky acanthapodia (Naegleria has more rounded pseudopods - see above). The middle image is a high power image of Acanthamoeba spp. cysts (note the hexagonal double cyst wall). The image on the right is a cyst seen using fluorescence. In these images, note the large karyosome with no peripheral nuclear chromatin.
Special thanks to the Centers for Disease Control and Prevention and the Armed Forces Institute of Pathology image collections for the images used in this case history.
References:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.