

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A patient is diagnosed as having diarrhea and 2 stool specimens are submitted to the laboratory. After examination of the concentration sediment from both specimens, nothing was seen and the results were reported as NO PARASITES SEEN. No permanent stained smears were prepared and/or examined. The patient continued to be symptomatic with GI problems and diarrhea. Would you agree or disagree with the original diagnostic approach? The patient submitted another stool specimen and both concentration sediment and permanent stained smears were examined. The parasites identified are seen below. If one considers all the intestinal protozoa, what organisms might have been missed without the permanent stained smear examination? What organism identification requires the permanent stained smear for identification? Why is this true? What references might be helpful in reviewing guidelines for a complete O&P examination?
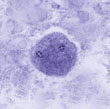
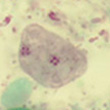
These protozoan trophozoites measure approximately 13 to 16 µm long. The one on the left is stained with iron hematoxylin; the one on the right is stained with trichrome. Hint: They are flagellates. Note that both trophozoites contain two fragmented nuclei.
Scroll Down for Answer and Discussion
Answer and Discussion of Quiz #3
The images presented in the Diagnostic Quiz are trophozoites of Dientamoeba fragilis; thus the physician's report (NO PARASITES SEEN) was incorrect.
D. fragilis was first seen in 1909 but not described until 1918. On the basis of electron microscopy studies, it has been reclassified as an ameba-flagellate rather than an ameba and is closely related to Histomonas and Trichomonas spp. It has a cosmopolitan distribution, and past surveys provide incidence rates of from 1.4 to 19%. Much higher incidence figures have been reported for mental institution inmates, missionaries, and Indians in Arizona. D. fragilis tends to be common in some pediatric populations, and in some studies, incidence figures are higher for patients under 20 years of age. Trophozoites can contain one or two nuclei, and the cyst is somewhat smaller with two nuclei (very difficult to identify since only about 1% of the forms will be cysts).
Although its pathogenic status is still not well defined, D. fragilis has been associated with a wide range of symptoms. Case reports of children infected with D. fragilis reveal a number of symptoms, including intermittent diarrhea, abdominal pain, nausea, anorexia, malaise, fatigue, poor weight gain, and unexplained eosinophilia. The most common symptoms in patients infected with this parasite appear to be intermittent diarrhea and fatigue. In some patients, both the organism and the symptoms may persist or reappear until appropriate treatment is initiated.
Diagnosis of D. fragilis infections depends on proper collection and processing techniques (a minimum of three fecal specimens). Although survival time for this parasite has been reported as 24 to 48 h, the survival time in terms of morphology is limited, and stool specimens must be examined immediately or preserved in a suitable fixative soon after defecation. It is particularly important that permanently stained smears of stool material be examined with an oil immersion lens (1,000 x). These organisms have been recovered in formed stool; thus, a permanent stained smear must be prepared for every stool submitted for a parasite examination.
If preserved specimens are submitted to the laboratory, it may be more cost effective to delete the direct smear and begin the stool examination with the concentration procedure, particularly since motile protozoa will not be viable because of the prior addition of preservative. Even if parasites are seen on a direct mount of preserved stool, they would almost certainly be seen on the concentration examination as well as on the permanent stained smear (protozoa in particular). With few exceptions, intestinal protozoa should never be identified on the basis of a wet mount alone; permanent stained smears should be examined to confirm the specific identification of suspected organisms.
Review
(Consistent with CAP Inspection Checklist): Every stool submitted for an O&P examination must be examined using the concentration and permanent stained smear procedures.
O&P Exam (Fresh Stool Specimen/liquid and/or very soft): Direct wet smear, concentration, permanent stained smear.
O&P Exam (Fresh Stool Specimen/formed stool): Concentration, permanent stained smear.
O&P Exam (Preserved Stool Specimen): Concentration, permanent stained smear.
Remember that all intestinal protozoan infections can be missed if the concentration ONLY is performed. The permanent stained smear is much more sensitive than the concentration alone. To date, there are no commercial immunoassay products available for the confirmation of infection with D. fragilis.
Additional Reading:
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.