

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
A 76-year old man was first seen in the clinic as a part of a routine examination. The stool was examined as an O&P exam with both a sedimentation wet examination and a permanent stained smear. No organisms were seen on the sedimentation concentration smear, but the following images represent what was seen on the permanent stained smear. The original case was seen at the Iowa State Hygienic Laboratory.
These images were examined using the oil immersion objective (100x oil immersion).
(Scroll Down for Answers and Discussions)
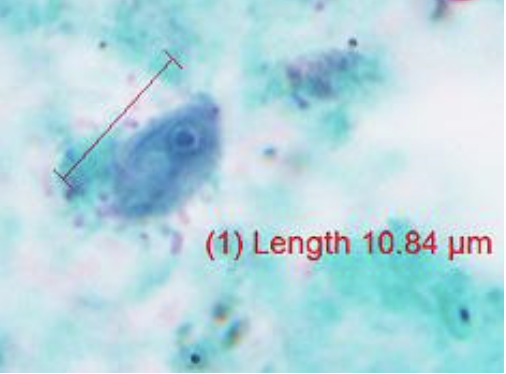
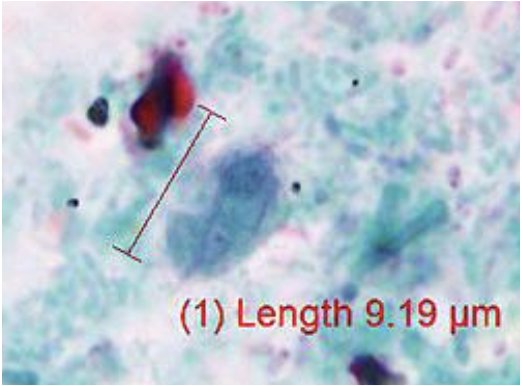
The images presented in Diagnostic Quiz #84 are the following:
These images contain Pentatrichomonas hominis trophozoites; measurements are seen above. Although this organism was not seen in the wet mount, additional morphology could be seen from the permanent stained slide examinations. This flagellate is considered nonpathogenic.
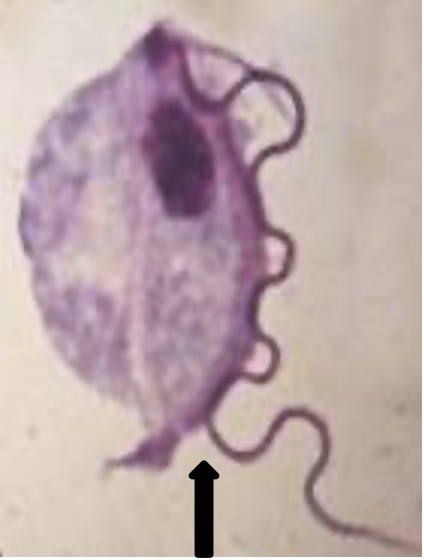
The genus name, Pentatrichomonas (Trichomonas), is based on the five anterior flagella and a granular parabasal body. P. hominis has been recovered from all parts of the world, in both warm and temperate climates. It is considered to be nonpathogenic, although it is often recovered from diarrheic stools. There is no known cyst stage. The trophozoites live in the cecal area of the large intestine and feed on bacteria. The organism is not considered to be invasive. The trophozoite measures 5 to 15 μm in length and 7 to 10 μm in width. It has a pyriform shape and has both an axostyle and undulating membrane, which help in the identification. The undulating membrane extends the entire length of the body, in contrast to that seen in Trichomonas vaginalis. Additional images are seen below; note undulating membrane comes all the way down the organism (unlike Trichomonas vaginalis in urinary-genital system which comes only half way down).

Routine stool examinations are normally recommended for the recovery and identification of intestinal protozoa. In freshly passed stool specimens, particularly in unformed stool, the motility may be visible. In a wet preparation, one specifically looks for the flagellar movement from the undulating membrane and the presence of the axostyle. These small flagellates are difficult to stain and may even be missed on a permanent stained smear, especially if the stain is pale. In more formed stools, the trophozoites may round up (not encysted) and may not exhibit the characteristic motility seen in more active forms. When preserved fecal specimens are received in the laboratory, the permanent stained smear is the most sensitive method for finding and identifying P. hominis.
MISDIAGNOSIS IN URINALYSIS:
It is important to remember that Trichomonas vaginalis is often diagnosed in urine via the organism motility. Since the finding of T. vaginalis in the urine of children can imply the possibility of a sexual transmission, it is very important to keep in mind the possibility of fecal contamination within a child’s urine due to collection issues. Thus P. hominis (nonpathogen in stool) could accidentally be misdiagnosed as T. vaginalis (pathogen / sexually transmitted flagellate) in urine. ANY DIAGNOSIS OF T. VAGINALIS IN A CHILD’S OR INFANT’S URINE SHOULD ALWAYS BE CONFIRMED; the misdiagnosis of P. hominis as T. vaginalis could be misinterpreted as a possible child abuse case.
EPIDEMIOLOGY AND PREVENTION:
Since there is no known cyst stage, transmission probably occurs in the trophic form. If ingested in a protecting substance such as milk, these organisms can apparently survive passage through the stomach and small intestine in patients with achlorhydria. P. hominis cannot be transplanted into the vagina, the natural habitat of T. vaginalis. Based on diagnostic test results, the incidence of this organism is relatively low, but it tends to be recovered more often than Enteromonas hominis or Retortamonas intestinalis. However, without the use of the permanent stained smear, the presence of P. hominis may be missed. The infection is diagnosed more often in warm climates and in children rather than adults. Because of the fecal-oral transmission route, preventive measures should emphasize improved hygienic and sanitary conditions. Although P. hominis is commonly found in dogs, puppies, and cats, there is no documented information related to possible transmission to humans.
TREATMENT:
Since P. hominisis nonpathogenic, there would be no necessity for treatment. However, if the patient remains symptomatic, it would be important to do additional testing for other possible pathogenic parasites, as well as other causes. In this particular case, the patient's symptoms are probably related to some other cause OR a true parasitic pathogen may be present and has not yet been identified (Example: Dientamoeba fragilis).
Garcia, L.S. 2016. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.
Garcia, L.S. 2009. Practical Guide to Diagnostic Parasitology, 2nd Ed., ASM Press, Washington, D.C.
Each Quiz has a two section format: the first section will present the Quiz topic and the second section will provide a discussion of the answer and/or various options in response to the Quiz situation presented to the user. In some situations, there may be more than one correct response.
The content within this site is made possible through the extensive contribution of Lynne S. Garcia, M.S., MT(ASCP), CLS(NCA), BLM(AAB), F(AAM), Director, Consultantation and Training Services (Diagnostic Medical Parasitology and Health Care Administration). For additional information, she can be contacted at LynneGarcia2@verizon.net.
Reference: Garcia, L.S. 2015. Diagnostic Medical Parasitology, 6th Ed., ASM Press, Washington, D.C.