Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
Fasciola gigantica (Pathogen – Liver Trematodes)
Organism:
Fasciola gigantica is closely related to F. hepatica. It is also a common parasite of cattle, camels, and other herbivores in Africa and of herbivores in some Pacific islands. Human infections have been reported in a number of areas of endemicity. Generally, F. hepatica is found in temperate zones and is the predominant species in Europe, the Americas, and Oceania, while F. gigantica is better adapted to tropical and aquatic environments and is the predominant species in Africa.
|
 |
 |
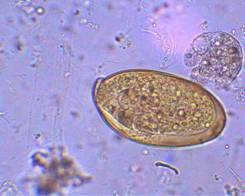
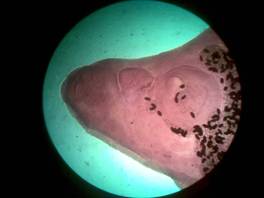
| Eggs (operculated) | X-section in liver |
 |
 |
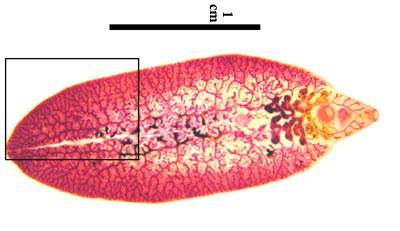
Adult worms
Life Cycle:
The life cycle is similar to that of F. hepatica; however, the snail hosts of F. gigantica are aquatic rather than amphibious like the first intermediate host for F. hepatica. Humans become infected through ingestion of water plants which carry the infective metacercariae. Apparently, developmental stages of F. gigantica grow at a slower rate, survive longer at high temperatures, and are more susceptible to drying than those of F. hepatica. The adult worm resembles F. hepatica but is somewhat more lanceolate, with a less distinct cephalic cone. The eggs are very difficult to differentiate from those of F. hepatica or Fasciolopsis buski; however, they tend to be larger (160 to 190 μm by 70 to 90 μm).
Acquired:
Humans are infected by ingestion of uncooked aquatic vegetation on which metacercariae are encysted.
Epidemiology:
Like F. hepatica, infection can occur in a wide range of herbivorous mammals when they ingest infected water plants or drink water contaminated with metacercariae. In some areas, the rate of infection in these animal hosts is quite high: in China, the rates are 50% for cattle, 45% for goats, and 33% for water buffalo; in Iraq, the rates are 71% for water buffalo and 27% for cattle; in northeastern Thailand, the rate is 60% for cattle. In various surveys, the occurrence of infections in cattle in Zambia was approximately 61%; in Tanzania the incidence in traditional, large-scale dairy and small-scale dairy cattle was 63.8%, 46.2% and 28.4%. Studies in Australia testing a commercially available ELISA for antibody detection was evaluated; results indicate this test will be very valuable in screening cattle and sheep for infections with F. hepatica, and probably F. gigantica.
Clinical Features:
The clinical symptoms of F. gigantica infection are very similar to those seen with F. hepatica and depend on the worm burden. The prepatent period between infection and the presence of adult worms in the bile ducts is 9 to 12 weeks. Patients may experience fever, nausea, vomiting, abdominal pain, hepatomegaly, hepatic tenderness, and eosinophilia. As in many light trematode infections, there may be vague symptoms or the patient may remain asymptomatic. Abscess or tumor‑like reactions have also been reported to occur in subcutaneous tissues or in the liver.
Clinical Specimen:
Stool: Confirmation of the infection depends on finding the operculated eggs in a routine stool examination; multiple stool examination may be required to find the eggs.
Laboratory Diagnosis:
Stool: The routine sedimentation concentration is recommended. Since the eggs are operculated they cannot be recovered from the zinc sulfate flotation method. The eggs of F. hepatica, Fasciolopsis buski, E. ilocanum, and G. hominis are similar in size and shape. Differentiation may be difficult without a patient history. Patients may be symptomatic during the first weeks of infection, but no eggs will be found in the stool until the worms mature, which takes 8 weeks. Multiple stool examinations may be needed to detect light infections.
Organism Description:
Egg: The eggs can be found in the stool; however, they may be absent more often than in infections with F. hepatica, so that multiple stool examinations may be required to demonstrate the eggs. Although these eggs are larger than those of F. hepatica or F. buski, they are very similar in shape. Recovery of adult flukes at surgery would confirm the diagnosis. Other diagnostic options as discussed with F. hepatica are also recommended for this infection.
Laboratory Report:
Fasciola typeeggs recovered
Treatment:
Although praziquantel is sometimes effective at a dose of 25 mg/kg taken after each meal for 2 days, it does not appear to be effective in treating patients in Egypt. Treatment with biothionol at 30 to 50 mg/kg on alternate days for 10 to 15 doses is recommended. Triclabendazole at 10 mg/kg as a single dose is also recommended, but this dose may not be as easily obtained. If a single dose has failed, the use of 20 mg/kg triclabendazole is recommended. The drug is given orally in single or multiple doses and has few side effects. It acts by inhibiting protein synthesis in F. hepatica and will probably become the drug of choice; however, it is not currently available in the United States unless possibly available through a compounding pharmacy.
Garcia, L.S. 2007. Diagnostic Medical Parasitology, 5th ed., ASM Press, Washington, D.C.
Control:
Prevention may be accomplished by public health education in areas where infections are endemic, stressing the dangers of eating watercress grown in the wild where animals and snails are abundant. Other measures have included killing snails, treating infected animals, and draining pasture lands.