

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
Enterobius vermicularis (Pinworm)(Pathogen – Intestinal Nematode)
Organism:
Enterobius vermicularis (pinworm) belongs to the nematodes, is a pathogen, and causes disease. E. vermicularis is thought to cause the world's most common human parasitic infection. It has been said, "You had this infection as a child; you have it now; or you will get it again when you have children!" The infection is more prevalent in the cool and temperate zones, where people tend to bathe less often and change their underclothes less frequently. Prevalence in children can be high, a fact that has been recorded despite the difficulties in confirming the infection.
 |
 |
 |
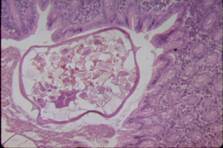 |
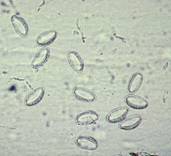
| Adult male and female Enterobius | Enterobius eggs | Enterobius adult worm | Adult worm, x-section of appendix |
Life Cycle:
Infection in humans is initiated by the ingestion of infective eggs, which hatch in the intestine (cecal region), where they develop into the adult worms. It probably takes about 1 month for the female to mature and begin egg production. After fertilization of the female worms, the males usually die and may be passed out in the stool. In gravid females, almost the entire body is filled with eggs. At this point, the female migrates down the colon and out of the anus, where the eggs are deposited on the perianal and perineal skin. Occasionally, the female worm migrates into the vagina. It is speculated that after egg deposition, the female worm returns to the intestine; however, this has not been proven.
Acquired:
Infection in humans is acquired through ingestion of infective eggs.
Epidemiology:
Worldwide; since this infection is so common and transmission is so easy (anus‑to‑mouth contamination, soiled nightclothes, airborne eggs, and contaminated furniture, toys, and other objects), prevention is marginal Recent studies also reveal that Enterobius infestation can occur in cockroaches, which may serve as potential reservoirs for these helminths and have considerable public health significance. Under most circumstances, total prevention is neither realistic nor possible.
Clinical Features:
Pinworm infection is the most common helminth infection within the United States and Western Europe; prevalence rates in some areas may be as high as 30 to 50%. The most striking symptom of this infection is pruritus, which is caused by the migration of the female worms from the anus onto the perianal skin before egg deposition. The sometimes intense itching results in scratching and occasional scarification. In most infected people, this may be the only symptom, and many individuals remain asymptomatic.
The degree of infection varies tremendously from patient to patient. As many as 5,000 worms have been removed from a single patient; however, most cases average less than one migrating worm per evening. Women are symptomatic three times as often as men and young people more frequently than older people.
Eosinophilia may or may not be present. Although tissue invasion has been attributed to the pinworm, these cases are not numerous. Infections tend to be more common in children and occur more often in females than in males. In heavily infected females, there may be a mucoid vaginal discharge, with subsequent migration of the worms into the vagina, uterus, or fallopian tubes, where they become encapsulated.
Although enterobiasis is an uncommon cause of acute appendicitis in children within the United States, this infection may be associated with acute appendicitis, chronic appendicitis, ruptured appendicitis, or with no significant symptoms.
Clinical Specimen:
Scotch Tape Prep: The standard O&P examination is NOT the recommended procedure for recovery and identification of E. vermicularis eggs. The cellulose tape (Scotch tape) preparation is recommended as the diagnostic test of choice (a minimum of four to six consecutive negative tapes is required to rule out the infection).
Laboratory Diagnosis:
Scotch Tape Prep: The cellulose tape (Scotch tape) preparation is recommended as the diagnostic test of choice (a minimum of four to six consecutive negative tapes is required to rule out the infection). Commercial paddles or other collection devices are also acceptable. Although the paraffin swab is also an option, this method is seldom used. Adult worms may be found on or under the surface of the stool specimen, particularly in children. The adult worms can also be found on the tapes. Eggs are occasionally recovered in stool, but this is an incidental finding.
Although the patient history of anal itching, irritability, and insomnia may suggest a pinworm infection, diagnosis depends on demonstrating the eggs or adult worms.
Organism Description:
Egg: The eggs have been described as footballs with one side flattened. They are oval, compressed laterally, and flattened on one side and measure 50 to 60 μm long by 20 to 30 μm wide.
Adult worm: The female worm measures 8 to 13 mm long by 0.3 to 0.5 mm wide and has a pointed tail (hence the name "pinworm"). The male is much smaller, measuring 2 to 5 mm long by 0.1 to 0.2 mm wide, and has a curved caudal end.
Laboratory Report:
Enterobius vermicularis eggs present.
Treatment:
Although several drugs such as pyrantel pamoate or mebendazole are extremely effective in eliminating the worms, the decision to treat should be based on evidence of infection and consideration of whether the patient is symptomatic. Repeat reinfection is always possible; thus, repeated treatment may need to be initiated to ensure that the patient is free of infection. Repeat treatment after about 2 weeks is routinely recommended to eliminate any infection acquired from ingestion of eggs that remain in the environment following the first treatment. Asymptomatic individuals are rarely treated, particularly in a group situation in which more susceptible individuals are not present. Treatment often includes counseling for the parents, who may be very upset at learning that their children have "worms." They may not realize how prevalent the infection is, particularly in children, and that many children will never have any symptoms or sequelae from the infection. In a group situation, often only one or several individuals will be symptomatic and continue to be infected. Treatment of the entire group, followed by retreatment of the more susceptible individuals, may provide an infection‑free group for a longer period.
Garcia, L.S. 2007. Diagnostic Medical Parasitology, 5th ed., ASM Press, Washington, D.C.
Control:
Under most circumstances, total prevention is neither realistic nor possible.