

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
Filariasis, Brugia malayi (Pathogen – Tissue Nematode)
Organism:
Infections are transmitted to humans by the bites of obligate blood‑sucking arthropods that had become infected through ingesting larvae (microfilariae) contained in a blood meal obtained from a mammalian host. The filarial nematodes are a group of arthropod‑borne worms that reside in the subcutaneous tissues, deep connective tissues, lymphatic system, or body cavities of humans. Some adult filarial worms can survive in the human host for many years, causing a number of chronic and debilitating symptoms, including inflammatory reactions.
 |
 |
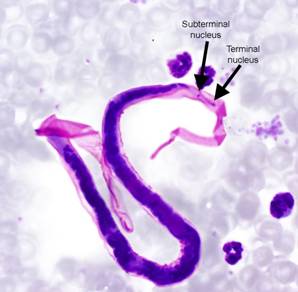 |
Brugia malayi microfilaria |
B. malayi tail nuclei |
 |
 |
 |
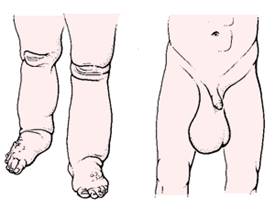
Various images of elephantiasis |
Life Cycle:
Although the two species can be differentiated morphologically, the life cycle of B. malayi is similar to that of W. bancrofti. However, Brugia has a shorter development time in the mosquito vector and the time from infection to appearance of microfilariae may be as short as 3 to 4 months. The adult worms inhabit the lymphatics, and the females give birth to sheathed microfilariae.
Acquired:
Infection in humans is acquired through the bite of infected mosquitoes.
Epidemiology:
There are two types of B. malayi, one nocturnally periodic and the other nocturnally subperiodic. The periodic strains, which have no animal reservoirs, are widely distributed in Asia, whereas the subperiodic form has been noted in Malaysia, Indonesia, and the Philippines. The principal mosquito vectors are Mansonia spp.; however, in certain areas Anopheles and Aedes spp. may be important. There are a number of reservoir hosts for B. malayi infections, including humans, dogs, cats, and monkeys.
Clinical Features:
Clinical manifestations usually develop months or years after infection, and many of the patients are asymptomatic even when they have microfilaremia. Lymphangitis and filarial abscesses occur with a greater degree of frequency than in W. bancrofti infections. If elephantiasis occurs, the swelling is normally restricted to the lower extremities below the knee. Sclerotic cordlike lymphatics and enlarged nodes in the arms and legs are common; urogenital involvement with chyluria does not occur. In disease caused by B. malayi, episodes of prolonged fever, adenolymphangitis, abscesses of affected lymph nodes, and local residual scarring occur quite frequently. Chronic lymphedema or elephantiasis, as seen in bancroftian filariasis, does not occur frequently.
Clinical Specimen:
Blood: In areas of endemic infection around the world, the presumptive diagnosis of filarial infections is frequently based on clinical evidence; however, definitive diagnosis is based on the detection of microfilariae, primarily in the blood.
Serum: Except for patients not native to the area of endemicity, immunodiagnostic tests are of limited value.
Laboratory Diagnosis:
Blood: The diagnostic methods are similar to those for W. bancrofti and include thin and thick blood films, wet preparations and concentrations, PCR, ultrasonography, antigen, and antibody detection.
Serum: Current tests lack both sensitivity and specificity, and most people from the region of endemicity will have a positive serologic response. This response may be due to exposure to nonhuman filarial antigens from infected mosquitoes, and filarial antigens may cross‑react with antibodies to other parasitic diseases.
Ultrasonography: Infection with B. malayi not only affects the structure and function of lymphatic vessels but also is associated with extralymphatic pathology and disease. Since it is now possible to detect living adult worms by ultrasonography, a great deal of emphasis is placed on lymphatic pathology. However, the finding of renal damage in asymptomatic microfilaremic carriers has led to increased recognition of the importance of extralymphatic complications in bancroftian filariasis. Filarial pathology of the male genitalia is apparently underreported if physical examination alone is evaluated.
Organism Description:
Adult: Adult worms are minute and threadlike, have a smooth cuticle, and are found in the lymph nodes and lymphatic channels.
Microfilariae: The microfilariae range from 177 to 230 μm long and actively move about in the lymph or blood. The microfilaria has a sheath, and there are two terminal nuclei that are distinctly separated from the other nuclei in the tail. There are nocturnally periodic and nocturnally subperiodic strains, so travel history can be helpful for optimal specimen collection times. Giemsa will stain the sheath pink.
Laboratory Report:
Serology results indicated (with interpretation); microfilariae identified and reported
Treatment:
The frequency of severe reactions is greater in B. malayi infections than in W. bancrofti infections. Initiation of treatment with lower doses of DEC and use of anti‑inflammatory drugs will reduce the adverse reactions. Ivermectin has also been used to treat B. malayi infections. Side effects are attributed to host response to the death of microfilariae rather than directly to the drug. Single doses are effective in clearing or reducing the microfilaremic burden for up to 6 months. However, a gradual decrease in microfilariae occurs over several weeks to 15 to 20% of pretreatment levels; this response is much slower than that seen with W. bancrofti and microfilariae clearance.
Garcia, L.S. 2007. Diagnostic Medical Parasitology, 5th ed., ASM Press, Washington, D.C.
Control:
Since these helminths do not multiply within the human host, infection levels are related directly to the number of infective larvae to which humans are exposed. Individual protection involves the use of insect repellents and bed netting; however, long‑term protection has been sought through vector control and the use of chemotherapy. Any prevention program must consider reservoir hosts other than humans in the control of B. malayi. Measures used for control and prevention have been similar to those used for W. bancrofti.