

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
African Sleeping Sickness (Trypanosoma brucei ssp., African Trypanosomiasis)
Organism:
Trypanosomes are hemoflagellates, which are transmitted by tsetse flies (Glossina spp.) to a wide range of mammalian hosts. They cause serious medical problems for humans and livestock. Trypanosomes belong to the family Trypanosomatidae that live in the blood and tissues of their human hosts. The African trypanosomes belong to the subgenus Trypanozoon and as a group are referred to as the Trypanosoma brucei complex. T. brucei brucei strains are parasites of domestic and wild animals and are not known to be infectious for humans. Human infections are caused by T. brucei gambiense (West African trypanosomiasis) and T. brucei rhodesiense (East African trypanosomiasis). Infections caused by T. brucei rhodesiense are much more fulminant than those caused by T. brucei gambiense, the parasitemia is much higher, and the disease has a much faster progression. It is not possible to differentiate the three trypomastigotes of T. brucei gambiense, T. brucei rhodesiense, and T. brucei brucei on the basis of morphology, and all three organisms can be recovered in animal reservoir hosts.
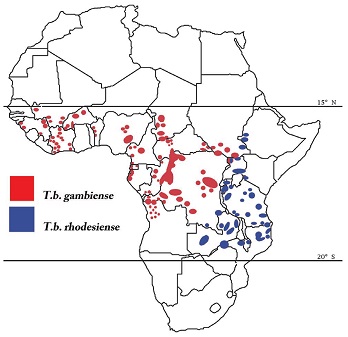
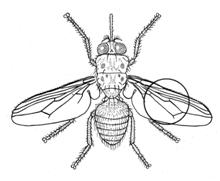



Upper Left: map for East and West African trypanosomiasis; Upper Right, diagram of Glossina, the tsetse fly; Lower Left and Middle, examples of the African trypomastigote (note the very small kinetoplast/circle); Lower Right, patient with sleeping sickness.
Life Cycle:
Trypanosomal forms are ingested by the tsetse fly (Glossina spp.) when a blood meal is taken. Once the short, stumpy trypomastigote reaches the midgut of the tsetse fly, it transforms into a long, slender procyclic stage. The organisms multiply in the lumen of the midgut and hindgut of the fly. After approximately 2 weeks, the organisms migrate back to salivary glands through the hypopharynx and salivary ducts, where the organisms attach to the epithelial cells of the salivary ducts and then transform to their epimastigote forms. In the epimastigote forms, the nucleus is posterior to the kinetoplast, in contrast to the trypomastigote, in which the nucleus is anterior to the kinetoplast. There is continued multiplication within the salivary gland, and metacyclic (infective) forms develop from the epimastigotes in 2 to 5 days. With development of the metacyclic forms, the tsetse fly becomes infective. During the act of feeding, the fly introduces the metacyclic trypanosomal forms into the next victim in saliva injected into the puncture wound. The entire developmental cycle in the fly takes about 3 weeks, and once infected, the tsetse fly remains infected for life.
Organism:
The trypanosomal (trypomastigote) forms can be found in the blood, cerebrospinal fluid (CSF), lymph node aspirates, and fluid aspirated from the trypanosomal chancre (if one forms at the site of the tsetse fly bite). The trypomastigote forms multiply by longitudinal binary fission. The organism is highly pleomorphic, having a variety of trypanosomal forms in the same blood smear. The forms range from long, slender-bodied organisms with a long flagellum (trypomastigote) that attain a length of 30 µm or more to short, fat, stumpy forms without a free flagellum that are approximately 15 µm long. The short, stumpy forms do not divide in the bloodstream but are the infective stage for the tsetse fly.
Antigenic Variation:
A unique feature of African trypanosomes is their ability to change the surface coat of the outer membrane of the trypomastigote, helping to evade the host immune response. The trypomastigote surface is covered with a dense coat of approximately 107 molecules of the membrane-form variant surface glycoprotein (VSG). There are approximately 100 to 1,000 genes in the genome, responsible for encoding as many as 1,000 different VSGs. More than 100 serotypes have been detected in a single infection. It is postulated that the trypomastigote changes its coat about every 5 to 7 days (antigenic variation). This change is responsible for successive waves of parasitemia every 7 to 14 days and allows the parasite to evade the host humoral immune response (4). There is no evidence that the host immune system induces the VSG switches. During antigenic switching, VSG is both internalized by the trypomastigote and released or shed into the blood. This shed VSG is most probably responsible for the immune dysfunctions noticed during infections. There is a release of gamma interferon (which stimulates parasite growth), suppression of interleukin-2, and hypergammaglobulinemia (very high levels of IgM).
Epidemiology:
T. brucei gambiense is transmitted from person to person by the bite of the tsetse fly (G. palpalis and G. tachinoides) after infectivity develops within the insect. The development cycle in the fly, depending on temperature and moisture, varies from 12 to 30 days and averages 20 days. Fewer than 10% of tsetse flies become infective after obtaining blood from infected patients, and vertical transmission from infected fly to offspring is not known to occur. G. palpalis and G. tachinoides can be found in areas of thick shrubbery and trees near the banks of rivers, streams, or water holes; therefore, transmission readily occurs when people frequent these areas. Both female and male tsetse flies can transmit the infection. In addition to biological transmission, the tsetse fly may mechanically transmit the infection with its proboscis if it bites an uninfected person within a few hours of biting an infected person. Congenital transmission in humans has also been documented.
Clinical Features:
In general, African trypanosomiasis caused by T. brucei gambiense (West African sleeping sickness) has a long, mild, chronic course that ends fatally with central nervous system (CNS) involvement after several years’ duration. This is unlike the disease caused by T. brucei rhodesiense (East African sleeping sickness), which has a short course and ends fatally within a year.
Stage I. After the host has been bitten by an infected tsetse fly, metacyclic trypomastigote stages are introduced into the skin, where they multiply and set up a local inflammatory reaction. A nodule or chancre at the site (3 to 4 cm) may develop after a few days. However, this primary lesion will resolve spontaneously within 1 to 2 weeks. The chancre is seen frequently in white Europeans but rarely in patients indigenous to an area where the disease is endemic.
Stage II. Once trypomastigotes invade the CNS, the sleeping sickness stage of the infection is initiated (stage II disease). The trypomastigotes are found primarily in the frontal lobes, pons, and medulla. Behavioral and personality changes are seen during CNS invasion. Gambian trypanosomiasis is characterized by steady progressive meningoencephalitis, apathy, confusion, fatigue, coordination loss, and somnolence (Figure 28.8). In the terminal phase of the disease, the patient becomes emaciated and progresses to profound coma and death, usually from secondary infection.
Laboratory Diagnosis:
Physical findings and clinical history are very important in establishing the diagnosis. Diagnostic symptoms include irregular fever, enlargement of the lymph nodes (particularly those of the posterior triangle of the neck [Winterbottom’s sign]), delayed sensation to pain (Kerandel’s sign), and erythematous skin rashes. However, diagnosing imported human African trypanosomiasis outside endemic areas is difficult and diagnosis is often delayed. Trypomastigotes may be detected in fluid aspirated from the ulcer. The trypomastigotes enter the bloodstream, causing a symptom-free low-grade parasitemia that may continue for months. This is considered stage I disease, where the patient can have systemic trypanosomiasis without CNS involvement. During this time, the parasites may be difficult to detect, even by thick blood film examinations. Many trypomastigotes may be found in the circulating blood during fevers, but few are seen during afebrile periods. Blood can be collected from either finger stick or venipuncture. Venous blood should be collected in a tube containing EDTA (fill the tube to obtain correct anticoagulant/blood ratio). Multiple slides should be made for examination, and multiple blood examinations should be done before trypanosomiasis is ruled out. Trypomastigotes can be aspirated from the enlarged lymph nodes. In addition to lymph node involvement, the spleen and liver become enlarged. With Gambian trypanosomiasis, the blood-lymphatic stage may last for years before the sleeping sickness syndrome occurs.
A simple and rapid test, the card indirect agglutination trypanosomiasis test (TrypTect CIATT), is available, primarily in areas of endemic infection, for the detection of circulating antigens in persons with African trypanosomiasis. The test is normally performed on a drop of freshly collected heparinized blood and is followed by a more specific confirmation test on diluted blood, plasma, or serum. The sensitivity of the test (95.8% for T. -brucei gambiense and 97.7% for T. brucei rhodesiense) is -significantly higher than that of lymph node puncture, microhematocrit centrifugation, and CSF examination after single and double centrifugation (16). Its specificity is excellent, and it has a high positive predictive value.
Treatment:
All drugs currently used in the therapy of African trypanosomiasis are toxic and require prolonged administration. Treatment should be started as soon as possible and is based on the patient’s symptoms and laboratory findings. The choice of antiparasitic drug depends on whether the CNS is infected. Suramin or pentamidine isethionate can be used when the CNS is not infected. Pentamidine is currently the drug of choice for the hemolymphatic stage with suramin being an alternate. Melarsoprol, a toxic trivalent arsenic derivative, is effective for both hemolymphatic and neural stages but is recommended for treatment of late-stage sleeping sickness. Eflornithine (dl-α-difluoromethylornithine; DFMO) has been used for more than 10 years to treat -melarsoprol-resistant T. brucei gambiense infection with or without CNS involvement; treatment is started intravenously and is followed by oral therapy.
Control:
Tourists are usually not at great risk unless they are traveling and spending long periods in rural areas of western and central Africa. Persons visiting areas where the disease is endemic should avoid tsetse fly bites by wearing protective clothing (long-sleeved shirts and long pants); khaki or olive-colored clothing is optimal, since the tsetse fly is attracted to bright colors and very dark colors. Because heavy clothing is not always practical owing to heat and humidity, other measures, including the use of insect repellents, bed netting, and screens, are recommended. It has also been recommended not to ride in the back of jeeps, pickup trucks, or other open vehicles; the tsetse fly is attracted to the dust created by moving vehicles and wild animals. Bushes should be avoided, since the tsetse fly is less active during the hot period of the day and rests in bushes but will bite if disturbed.