

Home
About Medical Parasitology
New Infections
Ova & Parasite (O&P) Exams
CPT Codes
Quizzes, General
Quizzes, Histology
Quizzes, Blood
Review Tests
FAQ
Information Tables
Organism Index (A-Z)
Angiostrongyliasis, Abdominal: Angiostrongylus (Parastrongylus) costaricensis (Pathogen - Tissue Nematode)
Organism:
Angiostrongylus costaricensis is a zoonotic parasitic nematode that causes abdominal or intestinal angiostrongyliasis in humans. It is endemic to the Americas. This parasite was first discovered in humans in Costa Rica. It is endemic to the Americas (from southern USA to northern Argentina in South America) and in humans causes abdominal or intestinal angiostrongyliasis, which mimics appendicitis with eosinophilia. The first reported outbreak of abdominal angiostrongyliasis occurred in Guatemala. Databases from 1996 to April 2012 revealed 27 case descriptions of abdominal angiostrongyliasis and 1 case series of 194 patients.
A. costaricensis mature adults usually live in mesenteric arteries of wild rodents, more commonly in Sigmodon hispidus and Rattus rattus. The nematode also requires terrestrial mollusks as intermediate hosts, especially from the family Veronicellidae. Children may accidentally eat slugs, or fruits and vegetables contaminated through mucoid secretions.

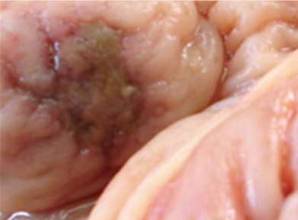

Angiostrongylus (Parastrongylus) costaricensis. Left, Slug and salad greens contaminated with infective larvae that have been shed by slugs in their mucus; Right, Necrotic ulcer in colonic mucosa; Bottom, worms in the ileocecal region of the natural rat host.
Life Cycle:
The life cycle is similar to that of A. cantonensis, with human infection being initiated by accidental ingestion of the appropriate slug, frequently on contaminated salad vegetables. This infection is called abdominal angiostrongyliasis, and the worms cause inflammatory lesions of the bowel wall. A. costaricensis requires two hosts: a vertebrate (the definitive hosts are rodents) and an invertebrate (the intermediate hosts are slugs and terrestrial mollusks). The first stage larvae (L1) are expelled in rodent feces, infecting mollusks orally and/or percutaneously. After two molting events, the larvae (L3) become infective. When rodents ingest mollusks infected with L3, the larvae penetrate the intestinal epithelium, closing the parasite life cycle. Humans can also be infected by the ingestion of L3 contaminated fruits, vegetables, raw food or water. Larvae migrate from the blood and lymphatic vessels to the heart, reaching the arterial circulation and subsequently the mesenteric arteries, where the parasites mature into the adult stage. The eggs are then deposited in the mesenteric arteries and are carried through the blood to the capillaries of the intestinal wall, where L1 will emerge to be expelled in feces.
Acquired:
Human infection begins with the accidental ingestion of infective larvae in several species of slugs and terrestrial mollusks and their mucus (contaminated salads, etc).
Epidemiology:
The ingestion of raw slugs in the areas of endemicity is considered strictly accidental. Most of the infections reported from Costa Rica have been in children, with a higher incidence in boys than in girls.
Clinical Features:
Patients suffering from this illness commonly have clinical signs similar to those of acute appendicitis. Sometimes intestinal obstruction, perforation and/or hemorrhage are found. A percentage of patients are ill for months, presenting relapsing episodes of abdominal pain. Often, patients exhibit leukocytosis and eosinophilia. The most common symptoms are pain and tenderness with fever, vomiting and diarrhea. A tumor-like mass is often palpable and can mimic malignancy. The symptoms of abdominal pain, vomiting and diarrhea, and anorexia, are often mistaken for those of appendicitis. Worms can be found in the regional lymph nodes and mesenteric arteries. They can also be found in the spermatic arteries causing testicular obstruction and necrosis. Occasionally the larvae and the ova reach the liver and symptoms may mimic visceral larvae migrans. Eosinophilia is also present.
Abdominal angiostrongyliasis in found mainly in children under 13 years, and some groups have reported that two-thirds of these are male. The appendix is often involved; however, the worms can also be found in the terminal ileus, cecum, ascending colon, regional lymph nodes, and mesenteric arteries. There may be inflammation, thrombosis, and regional necrosis, with granulomas and areas of eosinophilic infiltrates around eggs and larvae in various stages of development. The most common symptoms are pain and tenderness, with a palpable mass in the lower right quadrant, along with fever and possibly vomiting and diarrhea. Occasionally, the worms are present in the liver; the symptoms may mimic those of VLM. Leukocytosis is present, with eosinophilia of up to 80%. Clinical symptoms occur about 2 weeks after infection and include abdominal pain in the right iliac fossa and right flank, fever, anorexia, vomiting, diarrhea, and constipation.
Clinical Specimen and Organism Description:
This infection is usually identified by finding larvae and/or eggs in human tissue. Radiology may reveal abnormalities in the terminal ileum, cecum, and ascending colon. Contrast medium studies show spasticity, filling defects, and irritability at the cecum and ascending colon. When the liver is involved, there may be leukocytosis and eosinophilia, as well as elevated liver enzyme levels. The eggs are oval and about 90 µm long, have a thin shell, and are unembryonated (they may be embryonated in humans, with some larvae being released from the egg).
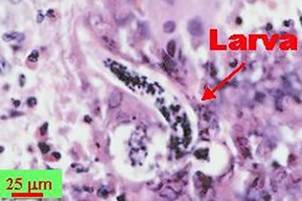

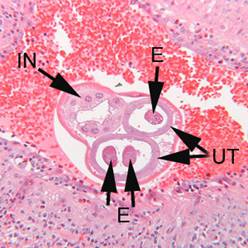
Left and Right, Angiostrongylus costaricensis larva and eggs in human intestinal tissue; Bottom, Female worm in appendix tissue; Notice the thick, multinucleate intestine (IN) and eggs (EG) within the uterus (UT). (Courtesy of the CDC Public Health Image Library).
Laboratory Diagnosis:
To date the diagnosis of abdominal angiostrongyliasis depends on the histological identification of Angiostrongylus costaricensis (AC) in surgical specimens. Lesions are most frequently found in the ileocecal region; however, localization in lymph nodes, omentum, liver, and testicles has also been observed. The presumptive diagnosis is made in the presence of severe eosinophilic infiltration, granulomatous reaction and eosinophilic vasculitis in the absence of parasitic structures. However, in the future PCR might help in the diagnosis of abdominal angiostrongyliasis, particularly when the pathologists are not experienced with such disease. Immunodiagnostic tests in serum have been developed, but show limitations due to cross-reaction with other parasite-related antibodies, such as Ascaris lumbricoides, Strongyloides stercoralis and Schistosoma mansoni
Treatment:
Several drugs have been tried; the drug of choice is thiabendazole, with another option being mebendazole. Depending on the clinical findings, surgical removal may be another option.
Control:
Prevention involves rodent control to break the normal parasite cycle, as well as thorough washing of vegetables and other foods prior to consumption.